The Hidden Muscle Change That Could Predict Type 2 Diabetes Years Before Diagnosis
Could muscle loss be raising your diabetes risk? Discover the latest evidence on sarcopenia, insulin resistance, and healthy aging.
DIABETESSARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/22/202622 min read
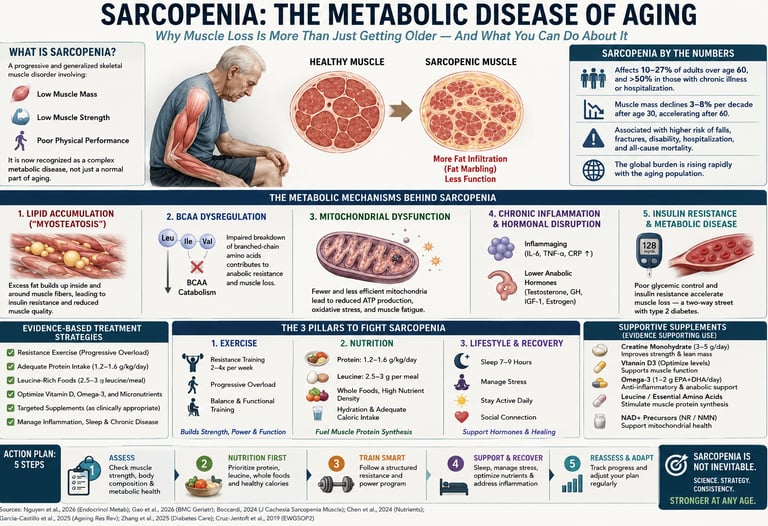
Yes. Sarcopenia and type 2 diabetes form a two-way relationship. Loss of muscle mass increases diabetes risk because skeletal muscle is the body's primary site of glucose disposal. Diabetes accelerates muscle loss through insulin resistance, inflammation, and mitochondrial dysfunction. Resistance training and adequate protein intake are the most evidence-based interventions for protecting both muscle and metabolic health.
Key points
1. Your muscle is a glucose-clearing organ, not just for strength
Skeletal muscle handles the majority of post-meal glucose disposal. Lose muscle mass or quality, and you lose a primary blood sugar buffer. That single mechanism links sarcopenia to diabetes risk before any lab value turns red.
2. The loop runs both ways, and it starts early
Prospective CHARLS data from 2026 shows changes in sarcopenia status predict new-onset T2DM. Even “possible sarcopenia” — low grip strength or slow gait speed alone — carried a ~27% higher 7-year diabetes risk. On the flip side, diabetes accelerates muscle decline via insulin resistance, AGE accumulation, and mitochondrial dysfunction.
3. Looking overweight doesn't mean you're safe
Sarcopenic obesity — low muscle hidden under excess fat — is one of the most underdiagnosed forms. Standard BMI or weight screens miss it. If you have T2DM, CKD, or are on weight-loss meds, assume you need a muscle check regardless of your pants size.
4. This combo compounds mortality risk
NHANES-based CKD data from 2026 found that when high cardiometabolic risk and sarcopenia co-exist, all-cause and cardiovascular mortality risk more than doubles. This isn’t additive risk. It’s multiplicative.
5. Imaging shows damage before diagnosis
DXA, CT, and MRI studies in T2DM patients reveal greater myosteatosis — fat infiltrating muscle — and lower muscle density before total mass drops enough to trigger standard sarcopenia criteria. Waiting for a formal diagnosis means waiting too long.
6. Resistance training is non-negotiable medicine
Aerobic exercise helps, but only resistance training directly stimulates muscle protein synthesis and increases GLUT4 density. For glucose control and muscle preservation, 2–3 sessions/week hitting all major muscle groups is the minimum effective dose. No supplement replaces mechanical load.
7. Protein strategy must be specific, especially on new weight-loss drugs
Target ~1.0–1.2 g/kg/day for at-risk adults, often 1.2–1.5 g/kg/day with confirmed sarcopenia or during rapid weight loss. Spread it across 3–4 meals at 25–35g each. GLP-1 agonists and SGLT2 inhibitors drive weight loss that can include lean mass — pair them with resistance training and protein by default, not as an afterthought.
8. Screen early, screen simply
You don’t need a DXA on day one. Handgrip strength, 5-times sit-to-stand test, and gait speed are validated, clinic-ready screens. Taking >15 seconds to stand 5x without using your arms is a red flag. If you have diabetes, prediabetes, or are 60+, make muscle screening as routine as an HbA1c.
Introduction
If you've been told to "watch your blood sugar," you've probably never been told to watch your muscle. Yet new research shows these two things are tangled together more tightly than almost anyone realized.
Sarcopenia — the progressive loss of muscle mass, strength, and physical performance — is no longer just an "old age" problem. It is now recognized as a genuine, bidirectional partner to type 2 diabetes mellitus (T2DM). Losing muscle raises your risk of developing diabetes. Having diabetes accelerates the loss of muscle. It's a feedback loop, and most people walking around with early signs of either condition have no idea it's happening.
This guide pulls together the most current peer-reviewed evidence — including large cohort studies from 2025 and 2026 — to answer the questions that matter most:
How exactly does losing muscle raise your risk of diabetes (and vice versa)?
What does the data actually show, and how strong (or shaky) is the evidence?
How do you find out if you already have early sarcopenia?
What specific, evidence-based actions actually move the needle on both muscle and glucose control?
What do the major health organizations recommend, and where is the science still uncertain?
What Is Type 2 Diabetes, in Muscle Terms?
You already know type 2 diabetes as a condition of high blood sugar driven by insulin resistance. What's less commonly explained is where most of your blood sugar actually goes after a meal.
Skeletal muscle is the single largest site of insulin-stimulated glucose disposal in the human body, accounting for the majority of glucose uptake after eating. In other words, your muscles are not just for moving — they are one of your body's primary glucose-clearing organs.
That single fact is the foundation of everything else in this article: if your muscle mass shrinks, or if the muscle you have becomes infiltrated with fat and stops responding properly to insulin, your body loses a major share of its glucose-disposal capacity. Blood sugar has fewer places to go, and that pushes you toward insulin resistance and eventually T2DM.
The Bidirectional Link: What the Science Actually Shows
Muscle Loss Predicting Future Diabetes
A 2026 prospective analysis of the China Health and Retirement Longitudinal Study (CHARLS) cohort examined how changes in sarcopenia status over time — not just a one-time snapshot — predicted who went on to develop new-onset T2DM (Gao et al., 2026). This is an important design upgrade over older cross-sectional studies, because it captures the trajectory of muscle decline rather than a single measurement.
This builds on earlier CHARLS-based work that had already shown a measurable signal: among adults aged 60+ who were diabetes-free at baseline, those classified with "possible sarcopenia" had roughly a 27% higher risk of developing new-onset T2DM over seven years of follow-up (hazard ratio approximately 1.27) compared with peers who had normal muscle function — a statistically significant finding even after adjustment for common confounders.
Why this matters clinically: This is not a small or borderline signal. A 27% relative increase in diabetes incidence, detected at the "possible sarcopenia" stage (i.e., before someone meets full diagnostic criteria), suggests muscle decline is an early, modifiable warning sign — arguably as useful as a fasting glucose creeping upward.
Diabetes Predicting Future Muscle Loss
The relationship runs the other way too. Long-standing clinical and mechanistic data — most recently synthesized in a 2026 expert position paper from a multidisciplinary international panel including geriatricians, endocrinologists, and nutrition specialists — describe how T2DM accelerates muscle decline through insulin resistance, chronic low-grade inflammation, oxidative stress, and prolonged hyperglycemia (Tarazona-Santabalbina et al., 2026).
The same paper highlights a critical clinical blind spot: sarcopenia is frequently underdiagnosed in people with diabetes, especially those who carry excess body fat — a presentation now commonly called sarcopenic obesity, where someone can look "overweight" on the scale while quietly losing functional muscle underneath.
The Combined Burden: Cardiometabolic and Kidney Consequences
The downstream stakes of this loop extend well beyond blood sugar numbers. A 2026 NHANES-based cohort study examined the Cardiometabolic Index (CMI) — a composite marker combining waist-to-height ratio and triglyceride-to-HDL ratio — together with sarcopenia status, in people with chronic kidney disease (CKD) (Zhang et al., 2026).
Among this CKD population, those in the highest CMI quartile had over double the risk of all-cause mortality (HR = 2.25) and over double the risk of cardiovascular mortality (HR = 2.03) compared with the lowest quartile, after full adjustment for confounders. Sarcopenia status independently tracked with worse survival curves in the same cohort.
Clinical translation: When poor muscle health and poor metabolic health occur in the same person — which is exactly the diabetes-sarcopenia overlap population — the mortality risk compounds rather than simply adding up. This is the real-world stakes behind the lab values.
Imaging Confirms the Structural Story
A 2026 imaging-focused review in Frontiers in Medicine consolidated what DXA, CT, MRI, and ultrasound studies show structurally in T2DM patients: greater intramuscular and intermuscular fat infiltration (myosteatosis), reduced muscle cross-sectional area, and lower muscle density compared with people without diabetes (He et al., 2026). Crucially, these structural changes can appear before a person loses enough total muscle mass to trigger a sarcopenia diagnosis on standard screening — reinforcing that mass-based screening alone may miss early disease.
A Global Pattern, Not Just an Asian or Western Phenomenon
It would be easy to assume this is a regional finding, given how many of the largest cohort studies (CHARLS, NHANES) come from China and the United States. A 2026 observational study of community-dwelling older adults in Ghana examined the risk of sarcopenia alongside bone turnover markers and broader metabolic health indices, finding consistent associations between musculoskeletal decline and metabolic dysfunction in a West African population (Kpabitey, 2026). This geographic spread strengthens confidence that the sarcopenia-metabolic link reflects a generalizable biological process rather than a population-specific artifact.
The Mechanisms: Why Muscle and Glucose Are So Connected
A comprehensive 2026 mechanistic review in Nutrition & Diabetes mapped out the overlapping biological pathways that drive this bidirectional relationship (Ghosh et al., 2026). Here is the cycle in plain language:
The "Vicious Cycle" Model
Step 1 — Muscle is your glucose sink. Skeletal muscle absorbs the majority of glucose after a meal via insulin-stimulated GLUT4 transporter activity. Less muscle mass means less storage capacity for incoming glucose.
Step 2 — Insulin resistance develops. As muscle shrinks or becomes infiltrated with fat (myosteatosis), the remaining tissue becomes less responsive to insulin signaling, so the pancreas compensates by producing more insulin — a state called hyperinsulinemia.
Step 3 — Chronic inflammation joins in. Both conditions are associated with elevated inflammatory markers, including C-reactive protein and pro-inflammatory cytokines such as TNF-alpha and IL-6, which independently impair muscle protein synthesis and worsen insulin signaling.
Step 4 — Hyperglycemia damages muscle directly. Chronically elevated blood glucose promotes the accumulation of advanced glycation end-products (AGEs), which stiffen connective tissue, impair mitochondrial function in muscle fibers, and accelerate protein breakdown.
Step 5 — Mitochondrial dysfunction reduces muscle quality. Diabetic muscle tends to show reduced mitochondrial density and oxidative capacity, which both lowers physical performance and worsens the muscle's ability to take up and burn glucose — looping back to Step 1.
Step 6 — Hormonal shifts compound the problem. Aging and diabetes both lower levels of anabolic hormones important for muscle maintenance, including insulin-like growth factor-1 (IGF-1), testosterone, and vitamin D, while also altering myokine (muscle-derived signaling molecule) output.
Shared Genetic and Cellular Signatures
Bioinformatics research has identified overlapping gene expression signatures and inflammatory pathways shared between sarcopenia and T2DM, particularly converging on mitochondrial function, oxidative phosphorylation, and immune-inflammatory signaling networks. This molecular overlap helps explain why the two conditions so often travel together rather than being coincidental comorbidities.
The Role of Drugs Used to Treat Diabetes
Not all glucose-lowering medications affect muscle the same way. Some research has flagged the theoretical and observed muscle-related effects of common diabetes drug classes:
Sulfonylureas: Associated with higher hypoglycemia risk, which over time may discourage physical activity and indirectly contribute to deconditioning.
SGLT2 inhibitors: Promote modest weight loss that can include some lean mass, raising clinical interest in pairing them with resistance training and adequate protein.
GLP-1 receptor agonists: Produce significant weight loss, a portion of which may also come from lean tissue, making muscle-preserving strategies especially relevant for patients on these drugs.
Metformin: Generally considered muscle-neutral or mildly favorable in most analyses, though data are still evolving.
This is a key practical point your doctor should know about: if you are losing significant weight on newer diabetes or weight-loss medications, ask specifically about resistance training and protein intake to protect muscle during that process.
How Strong Is the Evidence? Interpreting the Studies Critically
Strengths of the Current Evidence Base
Large, nationally representative cohorts. CHARLS and NHANES both sample tens of thousands of participants with standardized protocols, reducing the risk that findings reflect one hospital's unusual patient population.
Prospective designs with real follow-up time. Studies tracking participants for 7+ years (rather than a single snapshot) allow researchers to establish that muscle decline genuinely precedes diabetes onset — addressing the classic "which came first" problem.
Consistent direction across independent populations. Findings pointing the same direction in Chinese, American, and West African cohorts, using different sarcopenia definitions, increase confidence that this is a real biological phenomenon rather than a statistical fluke in one dataset.
Mechanistic plausibility. The epidemiological associations line up with well-established muscle physiology (insulin-stimulated glucose disposal, AGE accumulation, mitochondrial dysfunction), which is exactly the kind of convergence that strengthens causal inference in observational research
.
Where You Should Stay Skeptical
Most data is observational, not randomized. Cohort studies show association and temporal sequence, but they cannot fully rule out unmeasured confounders (e.g., undiagnosed early diabetes already subtly affecting muscle before "baseline" was measured).
Definitions of sarcopenia vary between studies. AWGS 2019, EWGSOP2, and various NHANES-derived proxy measures (like appendicular skeletal muscle mass index) don't always classify the same person the same way, which can make hazard ratios across studies harder to compare directly.
Self-reported diabetes status introduces noise. Some large surveys rely partly on self-report or single fasting glucose readings rather than oral glucose tolerance testing, which can undercount or miscategorize early diabetes.
Single-cohort effect sizes can be unstable. Some published hazard ratios for mortality in subgroup analyses came from relatively small final analytic samples (in the hundreds to low thousands after exclusions), which widens confidence intervals and should temper how strongly any single number is interpreted.
Sarcopenic obesity may be undercounted. Several mechanistic reviews flag that standard BMI- or mass-based screening can miss sarcopenia in people carrying excess fat, meaning some studies may underestimate true prevalence and, by extension, underestimate the strength of the association.
Most large cohorts skew older and come from specific regions. Generalizing findings from a 60+ Chinese cohort or a US NHANES sample to, say, a 40-year-old in a different country should be done cautiously, even though the Ghana cohort data is reassuring on this front.
The Bottom-Line Clinical Read
Taken together, the totality of evidence — consistent direction, biological plausibility, multiple populations, and prospective designs — supports treating sarcopenia as a genuine, modifiable risk factor for type 2 diabetes (and vice versa), even though no single study proves causation with the certainty of a randomized controlled trial. This is similar to how the medical field treats many other well-established risk factors (like physical inactivity and cardiovascular disease) that are hard to study with RCTs for ethical and practical reasons.
What this means for you: You don't need a perfect, unimpeachable study to justify acting on this. The signal is strong enough, consistent enough, and mechanistically grounded enough that protecting your muscle is a reasonable, low-risk, high-upside health priority — regardless of whether you currently have prediabetes, established diabetes, or neither.
Are You at Risk? Signs, Screening, and Diagnosis
Early Warning Signs (Don't Wait for a Formal Diagnosis)
Struggling to open jars, carry groceries, or stand up from a low chair without using your hands
Noticeably weaker grip strength compared to a few years ago
Slower walking pace, especially compared to people your age
Unintentional loss of muscle definition, even if your weight is stable or rising
Frequent fatigue after light physical tasks
Falls or near-falls that didn't used to happen
Who Should Get Screened
Consider asking your doctor for a sarcopenia and metabolic screen if you:
Are over age 60 (or over 50 with diabetes risk factors)
Have type 2 diabetes, prediabetes, or a strong family history of T2DM
Have unexplained weight changes, especially weight loss with stable or rising waist circumference
Have chronic kidney disease, given the demonstrated mortality stakes shown in CKD-specific cohorts
Are taking medications associated with significant weight loss (GLP-1 receptor agonists, SGLT2 inhibitors)
How Doctors Actually Diagnose It
Test What It Measures Typical Setting SARC-F questionnaire Self-reported strength, walking, rising, stair climbing, falls Quick in-office screen Handgrip dynamometry Muscle strength Clinic or even some pharmacies Gait speed test Physical performance Clinic hallway, 4-meter walk DXA scan Appendicular skeletal muscle mass Hospital or specialized clinic Bioelectrical impedance analysis (BIA) Estimated muscle/fat mass Many gyms and clinics CT or MRI Muscle cross-sectional area and fat infiltration (myosteatosis) Specialist/research settings
A simple self-check you can do today: Try to stand up from a hard, armless chair five times in a row as quickly as possible, without using your hands. Taking longer than about 15 seconds, or needing to use your arms, is a recognized red flag worth discussing with your doctor.
Evidence Summary Table: Key Studies at a Glance
Gao et al., 2026 (CHARLS)
Study Population / Design: Prospective cohort study tracking Chinese adults aged 45 and older.
Key Finding: Changes in a person's sarcopenia status over time successfully predicted incident Type 2 Diabetes Mellitus (T2DM).
Clinical Relevance: Confirms that the continuous trajectory of muscle decline matters for diabetes risk, rather than just a single baseline snapshot.
Related CHARLS Analysis (2023)
Study Population / Design: Longitudinal study tracking 3,707 adults aged 60 and older over a 7-year follow-up period.
Key Finding: "Possible" sarcopenia correlates with an approximate 27% higher risk of developing new-onset T2DM (Hazard Ratio ≈ 1.27).
Clinical Relevance: Demonstrates that even early, subclinical muscle decline carries a measurable, significant risk for diabetes.
Zhang et al., 2026 (NHANES, CKD Cohort)
Study Population / Design: Observational study utilizing NHANES participants diagnosed with Chronic Kidney Disease (CKD).
Key Finding: Patients in the highest Cardiometabolic Index (CMI) quartile had a 2.25 times higher risk of all-cause mortality and a 2.03 times higher risk of cardiovascular mortality compared to those in the lowest quartile.
Clinical Relevance: Highlights that combined metabolic and muscle dysfunction sharply accelerates mortality risk in patients already managing CKD.
Tarazona-Santabalbina et al., 2026
Study Population / Design: International expert consensus paper.
Key Finding: Proposes a newly integrated muscle screening and targeted nutrition protocol specifically designed for individuals living with diabetes.
Clinical Relevance: Establishes the first major multidisciplinary clinical roadmap aimed at bridging endocrinology and geriatric muscle care.
Ghosh et al., 2026
Study Population / Design: Mechanistic literature review.
Key Finding: Maps out the shared biological pathways connecting muscle and metabolic loss, specifically focusing on insulin resistance, chronic inflammation, advanced glycation end-products (AGEs), and mitochondrial dysfunction.
Clinical Relevance: Decodes the underlying biological "why" that explains observed epidemiological links.
He et al., 2026
Study Population / Design: Imaging review analyzing data from DXA, CT, MRI, and ultrasound studies in T2DM.
Key Finding: Patients with T2DM exhibit significantly greater myosteatosis (fat infiltration within the muscle) and overall reduced muscle quality compared to non-diabetic controls.
Clinical Relevance: Proves that structural muscle damage and quality degradation can happen well before a formal sarcopenia diagnosis is triggered.
Kpabitey, 2026 (Ghana)
Study Population / Design: Observational study focusing on community-dwelling older adults in Ghana.
Key Finding: Sarcopenia risk is directly linked to specific bone turnover markers and broader metabolic health indices.
Clinical Relevance: Confirms that the muscle-metabolism connection is a global reality that generalizes beyond exclusively Asian or Western cohorts.
Summary of Core Clinical Themes
Track Progression, Not Just Baseline: Healthcare providers must track the velocity of muscle loss over time, as progressive decline is a strong predictor of metabolic failure.
Look Beyond Bulk: Muscle quality (avoiding fat infiltration/myosteatosis) is just as critical as muscle mass. Structural damage often occurs silently before actual wasting is visible.
Screen Early: Because "possible" or subclinical sarcopenia significantly boosts diabetes risk, muscle screening should be integrated into routine mid-life and geriatric primary care.
Multidisciplinary Approach Required: Managing the intersection of muscle wasting, diabetes, and complications like CKD requires coordinated care plans bridging nutrition, endocrinology, and nephrology.
.
Practical Application: A Step-by-Step Muscle-Protection Protocol
This is where the science becomes action. Use this as a starting checklist — always personalize with your physician or a registered dietitian, especially if you have kidney disease, cardiovascular disease, or are on insulin.
Step 1: Get a Baseline
Ask for a handgrip strength test and gait speed assessment at your next visit
Request HbA1c, fasting glucose, kidney function (eGFR), and lipid panel
If accessible, ask about a DXA or BIA body composition scan
Step 2: Set Two Numbers as Targets
Protein target: generally 1.0–1.2 g/kg of body weight per day for older adults at risk of sarcopenia (higher end, around 1.2–1.5 g/kg, often recommended for those with confirmed sarcopenia or during intentional weight loss — confirm your personal target with a dietitian, especially if you have kidney disease)
Resistance training target: at least 2 non-consecutive days per week of structured resistance exercise hitting all major muscle groups
Step 3: Build the Weekly Structure
Day Focus Mon Resistance training (lower body emphasis) Tue Brisk walk or light cardio + protein-focused meals Wed Resistance training (upper body emphasis) Thu Rest or gentle mobility work Fri Resistance training (full body) Sat Active recovery (walking, swimming, cycling) Sun Rest, meal prep, weekly check-in on protein/activity log
Step 4: Recheck Every 3–6 Months
Track grip strength, gait speed, HbA1c, and body composition at consistent intervals to see whether your interventions are actually working — not just whether you "feel" stronger.
Important safety note: If you have advanced kidney disease, uncontrolled cardiovascular disease, or recent fractures, get medical clearance before starting any new resistance training program, and discuss safe protein limits, since high-protein intake requires individualized adjustment in significant kidney impairment.
Nutrition Strategy for Sarcopenia + Diabetes
Protein: Quality and Timing Matter, Not Just Quantity
Spread protein across 3–4 meals (roughly 25–35 g per meal) rather than loading it all at dinner — this better stimulates muscle protein synthesis throughout the day.
Prioritize leucine-rich protein sources (eggs, dairy, poultry, fish, soy, legumes) since leucine is a key trigger for muscle protein synthesis.
For those struggling to reach targets through food alone, oral nutritional supplements — including diabetes-specific formulations and those enriched with beta-hydroxy-beta-methylbutyrate (HMB) — have shown benefit for muscle strength outcomes in clinical nutrition research, though individual results vary and these should complement, not replace, real food.
Carbohydrate Quality
Favor high-fiber, lower-glycemic-index carbohydrates (legumes, whole grains, non-starchy vegetables) to support steadier blood glucose, which in turn reduces the AGE-driving spikes that damage muscle tissue over time.
Pair carbohydrates with protein and fiber at each meal to blunt post-meal glucose spikes.
micronutrients Worth Discussing With Your Doctor
Vitamin D: Frequently low in people with both sarcopenia and diabetes; deficiency is associated with worse muscle outcomes.
Omega-3 fatty acids: Some research suggests anti-inflammatory benefits relevant to both conditions.
Magnesium: Plays a role in both insulin sensitivity and muscle function; deficiency is common in poorly controlled diabetes.
Visual suggestion: A simple plate-method graphic adapted specifically for this population — half non-starchy vegetables, a palm-sized lean protein portion, a fist-sized portion of high-fiber carbohydrate, and a thumb of healthy fat.
Exercise Strategy for Sarcopenia + Diabetes
Why Resistance Training Is Non-Negotiable
Aerobic exercise is excellent for cardiovascular health and modest glucose improvements, but resistance training is the single most directly muscle-building intervention available, and it independently improves insulin sensitivity by increasing GLUT4 transporter density in trained muscle.
A Sample Beginner-Friendly Resistance Routine
(Always start lighter than you think you need and progress gradually; consult a physical therapist or trainer experienced with older adults or chronic disease populations if you're new to this.)
Lower body: Bodyweight or chair-assisted squats, step-ups, seated leg press
Upper body: Resistance band rows, wall or incline push-ups, seated shoulder press
Core/stability: Standing marches, modified planks, balance work (e.g., single-leg stance near a support)
Aim for 2–3 sets of 8–12 repetitions per exercise, 2–3 times per week, increasing resistance gradually as strength improves (a principle called progressive overload).
Don't Skip Aerobic and Balance Work
Aerobic exercise (150 minutes/week of moderate intensity, per general physical activity guidelines) supports cardiovascular health and modest additional glycemic benefits.
Balance training reduces fall risk, which is especially important since sarcopenia and diabetes both independently raise fall and fracture risk.
Common Myths and Mistakes
Myth 1: "I'm not skinny, so I can't have sarcopenia." False. Sarcopenic obesity — low muscle mass hidden under excess fat — is one of the most underdiagnosed presentations, precisely because people and even some clinicians associate muscle loss with being thin.
Myth 2: "Cardio alone will fix this." Aerobic exercise is valuable, but it does not stimulate muscle protein synthesis the way resistance training does. Relying on cardio alone, especially during a calorie deficit, can accelerate lean mass loss.
Myth 3: "More protein is always better, no limit." Not true for everyone. People with significant kidney impairment need individualized, often more conservative, protein targets — this is a conversation for your nephrologist or dietitian, not a one-size-fits-all rule.
Myth 4: "If my HbA1c looks fine, my muscles must be fine too." Glycemic control and muscle health are related but not identical. Someone can have reasonably controlled blood sugar while still losing significant muscle mass and strength, especially on weight-loss-promoting diabetes medications.
Myth 5: "Sarcopenia is just an inevitable, untreatable part of aging." Multiple consensus bodies, including the Global Leadership Initiative on Sarcopenia, now classify sarcopenia as a "potentially reversible" muscle disease, not an unstoppable decline — meaning targeted nutrition and resistance training genuinely change the trajectory for many people.
Myth 6: "Supplements can replace exercise." Protein powders, HMB, and other supplements may support muscle maintenance, but none of the current evidence suggests they work as a substitute for actual mechanical loading (resistance exercise).
Frequently Asked Questions
Q1: Can sarcopenia actually cause type 2 diabetes, or does diabetes just cause sarcopenia? The relationship is bidirectional. Prospective cohort data shows muscle decline (including "possible sarcopenia") predicting future diabetes onset, while separate mechanistic and clinical evidence shows established diabetes accelerating muscle loss. Most experts now describe this as a self-reinforcing cycle rather than a one-way causal arrow.
Q2: At what age should I start worrying about sarcopenia if I have diabetes? Muscle decline can begin as early as your 30s and accelerate notably after 60, but having diabetes — at any age — appears to accelerate this timeline. Discuss baseline strength and body composition screening with your doctor starting in your 40s and 50s if you have diabetes or strong risk factors for it.
Q3: What is "diabetic sarcopenia" — is it an official diagnosis? "Diabetic sarcopenia" is an increasingly used clinical term describing sarcopenia occurring specifically in the context of diabetes, with proposed dedicated screening protocols from expert panels, though it is not yet a universally standardized, separately coded diagnosis in all classification systems.
Q4: Can resistance training lower my blood sugar even without weight loss? Yes. Resistance training increases glucose uptake capacity in trained muscle independent of weight change, by increasing GLUT4 transporter activity and overall muscle glucose disposal capacity.
Q5: I'm on a GLP-1 medication and losing weight fast — should I worry about my muscles? This is a legitimate concern, since a portion of rapid weight loss on these medications can come from lean tissue. Prioritizing adequate protein intake and resistance training during treatment is a reasonable, evidence-informed precaution — discuss specifics with your prescribing physician.
Q6: Does sarcopenia increase my risk of diabetic complications, like kidney disease? Cohort data in chronic kidney disease patients shows that combined poor metabolic and muscle health markers are associated with substantially higher all-cause and cardiovascular mortality risk compared with either factor alone.
Q7: What's the fastest way to check if I might have sarcopenia at home? Try the five-times sit-to-stand test (rising from a hard chair five times without using your hands) and time it. Struggling to complete it in roughly 15 seconds, or needing your hands, is a recognized warning sign worth raising with your doctor.
Q8: Is muscle loss reversible once you have type 2 diabetes? In many cases, yes, to a meaningful degree. Structured resistance training combined with adequate protein intake has been shown in clinical nutrition studies to improve grip strength and other muscle parameters in older adults with T2DM, even though full reversal to a younger baseline isn't always realistic.
Q9: Do diabetes medications themselves cause muscle loss? Some classes (particularly those associated with significant weight loss, like GLP-1 receptor agonists and SGLT2 inhibitors) can contribute to some lean mass loss as part of overall weight reduction; others (like metformin) are generally considered muscle-neutral. This is an evolving area of research — bring it up directly with your prescriber.
Q10: How much protein do I actually need if I have both conditions? Many experts suggest 1.0–1.2 g/kg/day as a general target for older adults at risk of sarcopenia, often higher (around 1.2–1.5 g/kg/day) for those with confirmed sarcopenia, but this must be individualized — especially if you have any degree of kidney disease, where higher protein intake requires medical guidance.
Q11: Can sarcopenia screening be done outside of a hospital? Yes — many gyms, physical therapy clinics, and some primary care offices can perform handgrip strength testing, gait speed assessment, and bioelectrical impedance analysis without needing a hospital-based DXA scan.
Q12: Is this link the same in every population, or just in Asian and American studies? While the largest cohorts come from China (CHARLS) and the United States (NHANES), a 2026 study in community-dwelling older adults in Ghana found a similar pattern of association between musculoskeletal decline and metabolic health, supporting the idea that this is a broadly generalizable biological relationship.
Conclusion and Action Steps
Sarcopenia and type 2 diabetes are not two separate problems that happen to coexist in aging bodies — they are two expressions of the same underlying metabolic and muscular decline, each one quietly making the other worse. The strongest, most current cohort and mechanistic evidence supports treating muscle health as a frontline, modifiable target for diabetes prevention and management, not an afterthought.
Your action checklist, starting this week:
Get tested. Ask your doctor about a handgrip strength test, gait speed assessment, and relevant bloodwork (HbA1c, fasting glucose, kidney function).
Try the sit-to-stand self-check described above as an immediate, free home screen.
Add two resistance training sessions to your week, even short ones, starting now rather than "someday."
Recalculate your protein target based on your body weight and kidney function, and spread it across your meals.
Re-test in 3–6 months to see real, measurable change — not just how you feel.
Loop in a professional. A registered dietitian and, where needed, a physical therapist or certified trainer experienced with chronic disease populations can personalize this plan safely.
This isn't about chasing a number on a scale. It's about protecting the tissue that, more than almost any other in your body, determines how well you'll manage your metabolic health for decades to come.
This article is for educational purposes and does not replace personalized medical advice. Please consult your physician or a registered dietitian before starting any new exercise or nutrition program, especially if you have diabetes, kidney disease, or other chronic health conditions.
Related Articles
Resistance Training for Sarcopenia: A Beginner's Workout Plan | DR T S DIDWAL
Sarcopenia & Cardiovascular Disease: How Poor Muscle Mass Predicts Mortality | DR T S DIDWAL
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained | DR T S DIDWAL
Sources and References
Gao, L., Chen, Y., Su, S., et al. (2026). Sarcopenia changes and incident type 2 diabetes mellitus: a prospective analysis of the CHARLS cohort. BMC Geriatrics, 26, 556. https://doi.org/10.1186/s12877-026-07169-4
Luo, C., Liu, R., Zhang, G., et al. (2023). Possible sarcopenia and risk of new-onset type 2 diabetes mellitus in older adults in China: a 7-year longitudinal cohort study. BMC Geriatrics. https://doi.org/10.1186/s12877-023-04104-9
Zhang, Z., Xing, Y., Zhang, F., Zhang, X., & Zhong, Y. (2026). Cardiometabolic index (CMI) and sarcopenia as predictors of all-cause and cardiovascular mortality in chronic kidney disease: a NHANES-based cohort study. Renal Failure, 48(1). https://doi.org/10.1080/0886022X.2026.2624299
Tarazona-Santabalbina, F. J., Giorgino, F., Donini, L. M., et al. (2026). Sarcopenia in Diabetes: A proposal on integrating muscle assessment and nutritional intervention in people living with diabetes. Diabetes Research and Clinical Practice, 238, 113326. https://doi.org/10.1016/j.diabres.2026.113326
Ghosh, M., Heo, Y., Kushwaha, G. S., et al. (2026). Interplay between sarcopenia and type 2 diabetes: mechanisms, implications, and therapeutic prospects. Nutrition & Diabetes. https://doi.org/10.1038/s41387-026-00431-z
He, L., Luo, G., Jiang, H., et al. (2026). Sarcopenia in type 2 diabetes mellitus: an imaging review. Frontiers in Medicine, 13, 1637499. https://doi.org/10.3389/fmed.2026.1637499
Kpabitey, I. L. (2026). Sarcopenia risk, bone turnover and metabolic health indices among community-dwelling older adults in Ghana: An observational study. Gerontology and Geriatric Medicine. https://doi.org/10.1177/30495334261456207
de Luis Román, D., Carretero Gómez, J., García-Almeida, J. M., et al. (2024). Diabetic Sarcopenia. A proposed muscle screening protocol in people with diabetes. Reviews in Endocrine and Metabolic Disorders. https://doi.org/10.1007/s11154-023-09871-9
Kim, M., & Kobori, T. (2023). Association of a Combination of Sarcopenia and Type 2 Diabetes with Blood Parameters, Nutrient Intake, and Physical Activity. Nutrients, 15(23), 4955.
Russo, C., Valle, M. S., Cambria, M. T., & Malaguarnera, L. (2025). Inflammatory Crosstalk Between Type 2 Diabetes and Sarcopenia: Insights from In Silico Evaluation. International Journal of Molecular Sciences, 26(16), 7932.
Carcelén-Fraile, M. C., Aibar-Almazán, A., Afanador-Restrepo, D. F., et al. (2023). Does an Association among Sarcopenia and Metabolic Risk Factors Exist in People Older Than 65 Years? A Systematic Review and Meta-Analysis. Life, 13(3), 648.
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., et al. (2019). Sarcopenia: revised European consensus on definition and diagnosis (EWGSOP2). Age and Ageing, 48(1), 16–31.
Chen, L. K., Woo, J., Assantachai, P., et al. (2020). Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. Journal of the American Medical Directors Association, 21(3), 300–307.
Donini, L. M., Busetto, L., Bischoff, S. C., et al. (2022). Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO Consensus Statement. Obesity Facts, 15(3), 321–335.
Park, S. W., Goodpaster, B. H., Lee, J. S., et al. Excessive loss of skeletal muscle mass in older adults with type 2 diabetes. Diabetes Care (Health, Aging, and Body Composition Study).
Sun, Q., Ren, Q., Du, L., et al. (2023). Cardiometabolic index (CMI), lipid accumulation products (LAP), waist triglyceride index (WTI) and the risk of acute pancreatitis. Lipids in Health and Disease, 22(1), 190.
de Luis Román, D., Vallo, F. G., Gómez, J. C., et al. (2023). Decreased muscle mass in type-2 diabetes. A hidden comorbidity to consider. Nutrición Hospitalaria, 40(1), 59–66.
Giha, H. A., Alamin, O. A. O., & Sater, M. S. (2022). Diabetic sarcopenia: metabolic and molecular appraisal. Acta Diabetologica, 59(8), 989–1000.
Identification of the shared gene signatures and pathways between sarcopenia and type 2 diabetes mellitus. (2022). PLOS ONE.
Sayer, A. A., & Cruz-Jentoft, A. (2022). Sarcopenia definition, diagnosis and treatment: consensus is growing. Age and Ageing, 51(10).
Larsson, S. C., et al. Genetically predicted insulin-like growth factor-I in relation to muscle mass and strength. Clinical Endocrinology.
Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. (2023). Metabolism: Clinical and Experimental.
Sarcopenia and type 2 diabetes: Pathophysiology and potential therapeutic lifestyle interventions. (2023). ScienceDirect / Diabetes and Metabolic Syndrome: Clinical Research and Reviews.
The Impact of Glucose-Lowering Drugs on Sarcopenia in Type 2 Diabetes: Current Evidence and Underlying Mechanisms. (2021). PMC.
Role of Medical Nutrition Therapy as Treatment of Sarcopenia in Older People with Type 2 Diabetes. PMC.
Effects of High-Protein Nutritional Guidance on Sarcopenia-Related Parameters in Individuals Aged ≥75 Years with Type 2 Diabetes. PMC (UMIN000044687 registered trial).
World Health Organization. Global recommendations on physical activity for health.
National Health and Nutrition Examination Survey (NHANES), Centers for Disease Control and Prevention. www.cdc.gov/nchs/nhanes/
China Health and Retirement Longitudinal Study (CHARLS) cohort profile. International Journal of Epidemiology.
Malnutrition, sarcopenia and nutrition therapy for patients with diabetes — A general framework and focus on hospital care. (2025). Clinical Nutrition ESPEN.