How Exercise Targets Atherosclerosis: From Prevention to Plaque Stabilization and Vascular Repair
Unlock the molecular benefits of exercise for heart disease prevention, including myokines, shear stress, and microRNA-driven vascular repair
EXERCISEHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/1/202614 min read
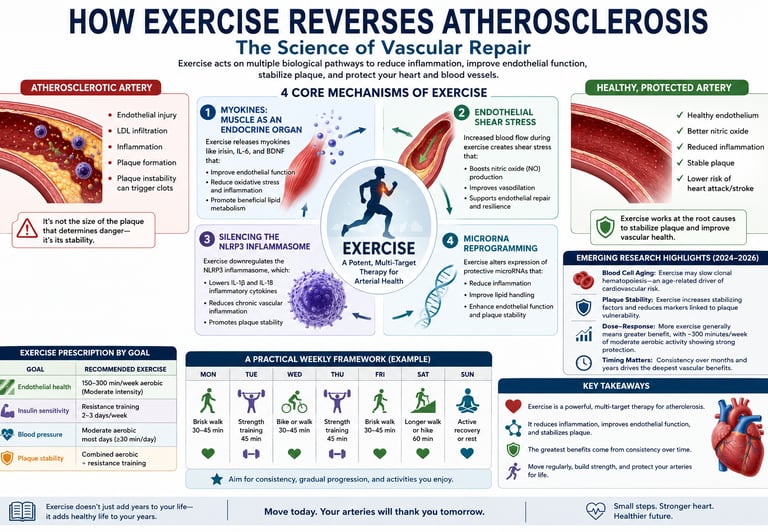
Exercise is not just prevention—it is molecular therapy for atherosclerosis.
Every workout triggers a cascade of protective signals inside your arteries, from anti-inflammatory myokines and improved endothelial function to suppression of plaque-destabilising pathways like the NLRP3 inflammasome. It also reshapes gene expression through microRNAs and reduces the burden of atherogenic ApoB-containing lipoproteins.
A 58-year-old man with hypertension, elevated LDL cholesterol, and coronary artery disease begins brisk walking 40 minutes five days per week plus two resistance sessions. Over six months, his blood pressure, exercise capacity, endothelial function, and inflammatory markers improve, illustrating how consistent training influences multiple biological pathways simultaneously
“Exercise reduces MACE risk by ~20–30% in longitudinal cohorts”
“VO₂ max improvement of 1 MET → ~10–15% mortality reduction”
“CRP reductions of ~20–40% with regular training”
Clinician’s Perspective
Exercise is not lifestyle advice—it is vascular pharmacology.
In modern cardiometabolic medicine, physical activity should be prescribed with the same intentionality as statins or antihypertensives. The difference is that exercise acts upstream, targeting the biology of disease initiation, not just downstream risk markers.Atherosclerosis is fundamentally inflammatory, and exercise is a multi-pathway anti-inflammatory therapy.
Beyond lipid-lowering, regular physical activity suppresses chronic low-grade inflammation through coordinated effects on cytokines, oxidative stress, and immune cell signalling. The inhibition of pathways such as the NLRP3 inflammasome represents a level of disease modification that most drugs only partially achieve.Endothelial function is the earliest and most reversible target.
Clinically, improvements in endothelial nitric oxide bioavailability occur within weeks of initiating aerobic exercise. This translates into better vasodilation, reduced arterial stiffness, and early plaque stabilization—well before structural changes are visible on imaging.ApoB particle burden—not just LDL-C—must frame our understanding.
Exercise favorably alters atherogenic lipoprotein dynamics by reducing ApoB-containing particle number and improving clearance. This is critical in patients with residual risk despite “normal” cholesterol levels.Skeletal muscle is an endocrine organ with systemic therapeutic reach.
Myokines such as irisin and exercise-induced IL-6 create an anti-inflammatory, metabolically favorable internal environment—linking muscle activity directly to vascular protection.Consistency outweighs intensity in long-term outcomes.
While high-intensity protocols amplify molecular responses, it is the chronic repetition of these signals—AMPK activation, mitochondrial adaptation, epigenetic modulation—that drives durable cardiovascular benefit.Exercise is most powerful when integrated, not isolated.
Combined aerobic and resistance training produces complementary effects across vascular, metabolic, and musculoskeletal systems—mirroring the multifactorial nature of atherosclerosis itself.The clinical shift is clear:
Exercise should move from being recommended to being prescribed, monitored, and followed up—as a first-line, disease-modifying therapy in cardiovascular care.For improving endothelial health: Aim for 150–300 minutes of moderate-intensity aerobic exercise per week, such as brisk walking, cycling, swimming, or jogging.
For enhancing insulin sensitivity: Perform resistance (strength) training at least 2–3 days per week, targeting all major muscle groups.
For lowering blood pressure: Engage in moderate-intensity aerobic exercise on most days of the week, ideally accumulating at least 30 minutes per day.
For promoting plaque stability and overall vascular protection: Combine regular aerobic exercise with resistance training, as both activate complementary biological pathways that support arterial health.
Introduction
Atherosclerosis develops silently for decades before it ever produces a symptom. By the time chest pain, breathlessness, or a cardiac event brings someone to a clinic, the underlying arterial changes have usually been building for twenty or thirty years.
That slow, hidden timeline is exactly why physical activity deserves to be talked about differently than it usually is. Exercise is rarely described with the same precision as a medication, yet a growing body of vascular biology research shows that it acts on the same disease pathways that drugs are designed to interrupt — inflammation, lipid handling, endothelial injury, and plaque instability.
This guide walks through what actually happens inside your arteries when you move: the signaling proteins your muscles release, the mechanical forces exercise creates inside blood vessels, the inflammatory switches it turns off, and the genetic reprogramming it triggers over months and years of consistent training. Along the way, you'll find a practical, evidence-informed weekly framework you can use regardless of your current fitness level.
What Is Atherosclerosis? A Quick Primer
Atherosclerosis starts with an injury — not a blockage. The innermost lining of an artery, called the endothelium, is a single layer of cells that normally keeps blood flowing smoothly and keeps immune cells out of the vessel wall.
High blood pressure, elevated LDL cholesterol, smoking, and chronic low-grade inflammation all damage this lining over time. Once it's compromised, LDL particles slip into the wall, immune cells follow, and a slow inflammatory response builds a fibrous, lipid-rich plaque. Plaques that grow large enough narrow the artery. Plaques that become unstable can rupture, triggering a clot — and a heart attack or stroke.
The critical point clinicians want patients to understand: it is not the size of a plaque that determines danger, it's its stability. A small, unstable plaque can rupture and kill; a larger, stable, calcified plaque may sit quietly for years. This distinction is central to why exercise matters so much — several of its mechanisms are specifically aimed at stabilization, not just "shrinking" plaque.
Why Exercise Is More Than "Lifestyle Advice"
In clinical cardiology, exercise still tends to be offered as a general recommendation rather than a prescribed, dosed intervention — something patients are told to "try to do more of," in the same breath as advice about eating vegetables.
That framing undersells what the biology actually shows. Statins, antihypertensives, and antiplatelet drugs each interrupt one part of the atherosclerotic process. Exercise engages several of these processes at once: it improves how much nitric oxide your blood vessels can produce, it changes the behavior of circulating immune cells, it shifts the composition of your cholesterol-carrying particles, and — more surprisingly — it appears to alter which genes your vascular cells express.
None of this makes exercise a replacement for medical therapy when medication is indicated. But it does support treating physical activity as a dosed, trackable, disease-modifying therapy rather than an optional add-on — something to be prescribed and followed up on, not just mentioned in passing.
Mechanism 1: Myokines — Muscle as an Endocrine Organ
Contracting skeletal muscle doesn't just burn fuel. It secretes signaling proteins called myokines directly into the bloodstream, where they act on the heart, liver, fat tissue, and blood vessels.
Irisin: The Vascular Guardian
Irisin is released when a membrane protein called FNDC5 is cleaved during aerobic activity. Research in ApoE-deficient mice — a standard model for atherosclerosis — found that exercise-driven irisin release tracked closely with better endothelial function and less plaque development <cite index="1-30">as demonstrated in a study showing aerobic exercise-induced irisin secretion is directly associated with improved endothelial function and reduced atherosclerotic lesion formation</cite>.
Mechanistically, irisin appears to work on several fronts at once: it dampens oxidative stress inside the vessel wall, quiets inflammatory signaling in endothelial cells, and supports nitric oxide production — the molecule primarily responsible for keeping arteries relaxed and resistant to plaque formation.
IL-6: The Anti-Inflammatory Paradox
Interleukin-6 (IL-6) has an unusual dual identity. Chronically elevated IL-6 — the kind seen in obesity and metabolic syndrome — tracks with higher cardiovascular risk. But the IL-6 released in short pulses during a workout behaves in the opposite direction: it's transient, and it stimulates production of anti-inflammatory signals like IL-10 and IL-1 receptor antagonist, which blunt the low-grade inflammation that drives plaque formation.
A systematic review and meta-analysis examining how different training styles affect myokine output found that exercise mode genuinely matters — aerobic training reliably produced strong, sustained irisin and IL-6 responses, while resistance training generated a distinct but complementary myokine signature <cite index="1-38,1-39">aerobic training was particularly effective at eliciting sustained irisin and IL-6 responses, while resistance training produced distinct myokine signatures with complementary benefits, showing that exercise type is a meaningful consideration for cardiovascular goals</cite>. In practice, this means the type of training you choose isn't arbitrary — different modalities appear to activate different protective pathways.
Mechanism 2: Endothelial Shear Stress — The Mechanical Signal
Chemistry isn't the only language your arteries respond to — physics matters too. As blood moves through a vessel, it drags against the endothelial surface, generating shear stress. Smooth, laminar flow produces a shear pattern that protects the endothelium. Turbulent or oscillatory flow — the kind that occurs naturally at arterial branch points — creates the opposite effect, and it's exactly where plaques tend to form first.
Aerobic exercise increases cardiac output and blood velocity, which raises laminar shear stress throughout the circulation. Endothelial cells physically sense this force through mechanoreceptors on their surface, and in response they upregulate an enzyme called eNOS, which produces more nitric oxide, reduces the expression of "sticky" adhesion molecules that recruit inflammatory cells, and lowers local oxidative stress.
The clinician's shorthand for this is useful: think of each aerobic session as a kind of internal polish for the vessel wall — a repeated mechanical signal that keeps the endothelial lining smooth, reactive, and resistant to the buildup that starts atherosclerosis.
Mechanism 3: Silencing the NLRP3 Inflammasome
The NLRP3 inflammasome is a protein complex inside immune cells that acts as an internal alarm system. When it detects oxidized LDL, cholesterol crystals, or metabolic stress — all present inside atherosclerotic lesions — it triggers release of IL-1β and IL-18, two cytokines strongly linked to plaque instability and rupture.
A detailed 2026 review examined the evidence that exercise interrupts this pathway through several converging routes:
Antioxidant enhancement — training boosts enzymes like superoxide dismutase and glutathione peroxidase, reducing the reactive oxygen species that activate NLRP3.
Autophagy stimulation — exercise triggers cellular "housekeeping" that clears damaged organelles and cholesterol crystals before they can trigger the inflammasome.
AMPK activation — this exercise-activated enzyme directly restrains NLRP3 priming, interrupting the inflammatory cascade upstream.
Improved mitochondrial function — reducing mitochondria-derived reactive oxygen species removes one of the main drivers of NLRP3 activity inside plaque macrophages <cite index="1-63">consistent with findings that regular exercise improves mitochondrial function and reduces mitochondrial-derived reactive oxygen species, removing a major driver of NLRP3 activation in macrophages within plaques</cite>.
Newer molecular work has refined this picture further. Research published in Life Sciences in 2026 looked specifically at how aerobic exercise stabilizes existing plaques, identifying a pathway involving suppression of a specific microRNA (miR-15a-5p) that normally represses a protein called Semaphorin-3A in the smooth muscle cells lining arteries — a mechanism directly tied to keeping plaques structurally stable rather than prone to rupture (Hu et al., 2026).
Because unstable plaques are what actually cause heart attacks — not simply plaque size — this NLRP3-focused research may represent one of the most clinically meaningful links between physical activity and the prevention of acute cardiac events.
Mechanism 4: MicroRNA Reprogramming of Vascular Genes
MicroRNAs (miRNAs) are small non-coding RNA molecules that fine-tune which genes get translated into protein. Exercise changes the levels of numerous circulating miRNAs, several with direct effects on vascular protection:
miR-126 — increased by exercise-driven shear stress, it supports endothelial repair and reduces the signals that recruit monocytes into the vessel wall.
miR-146a — acts as a brake on the NF-κB inflammatory pathway, reducing adhesion molecule expression on endothelial cells.
miR-21 — modulated by aerobic training, it influences whether smooth muscle cells in plaques stay quiescent or shift toward a more proliferative, lesion-advancing state <cite index="1-90">work summarizing this area highlights that miR-21 is modulated by aerobic training and plays complex roles in smooth muscle cell behaviour within plaques, influencing their phenotypic switching from a quiescent to a proliferative state — a critical step in lesion progression</cite>.
What makes this layer of biology distinct is that its effects can outlast any single workout. Regular training appears to reshape how vascular genes are expressed over time — a kind of biological memory written into gene regulation rather than DNA sequence itself.
Emerging Research: Blood Cell Aging, Plaque Stability, and Dose-Response
The last two years have added several new layers to this picture, moving the field beyond broad mechanisms toward more specific, clinically oriented questions: how much exercise, at what intensity, and through which additional pathways.
Clonal hematopoiesis and blood cell aging. One of the more unexpected recent findings connects exercise and sleep to a process called clonal hematopoiesis — the age-related expansion of mutated blood stem cell clones that has been independently linked to elevated cardiovascular risk. Emerging research suggests that adequate sleep combined with regular exercise may help limit the expansion of these pro-inflammatory clones, offering a plausible new explanation for part of exercise's cardioprotective effect (Huynh, 2026). This line of work is still early, but it broadens the conversation about exercise and atherosclerosis beyond the vessel wall itself, into how blood cells are produced and age over a lifetime.
Dose-response in people with overweight and obesity. A 2026 Bayesian meta-analysis of randomized controlled trials focused specifically on continuous aerobic exercise and vascular health markers in adults with overweight or obesity — a population at disproportionately high atherosclerosis risk. This kind of dose-response modeling helps answer a question patients ask constantly: not just whether exercise helps, but how much is needed to move vascular risk markers in a population that often has the most to gain (Bian et al., 2026).
Plaque-level mechanisms. As noted above, the 2026 Life Sciences study on miR-15a-5p and Semaphorin-3A adds a specific molecular explanation for how aerobic exercise physically stabilizes existing plaque structure at the level of vascular smooth muscle cells — moving the field from "exercise reduces inflammation" toward a more precise account of how a plaque becomes less likely to rupture (Hu et al., 2026).
Taken together, this newer research doesn't overturn the earlier myokine–shear stress–inflammasome–microRNA framework; it fills in the gaps around it, connecting exercise to processes as varied as bone marrow biology and the structural integrity of an individual plaque.
Evidence Summary Table
1. Myokine Signaling
Key Players: Irisin, IL-6
What It Does: Reduces oxidative stress, boosts nitric oxide production, and triggers the release of anti-inflammatory cytokines.
Representative Source: Inoue et al., 2026; Bettariga et al., 2024
2. Endothelial Shear Stress
Key Players: eNOS (Endothelial nitric oxide synthase), nitric oxide
What It Does: Improves vasodilation (widening of blood vessels) and suppresses adhesion molecules to prevent plaque buildup.
Representative Source: Yin & Guo, 2025
3. NLRP3 Inflammasome Suppression
Key Players: AMPK, autophagy, mitochondria
What It Does: Stabilizes arterial plaque and reduces the release of pro-inflammatory cytokines like IL-1β and IL-18.
Representative Source: Liu et al., 2026; Hu et al., 2026
4. MicroRNA Reprogramming
Key Players: miR-126, miR-146a, miR-21
What It Does: Epigenetically shifts vascular gene expression to promote cellular and tissue repair.
Representative Source: Ke et al., 2025
5. Blood Cell Aging Mitigation
Key Players: Clonal hematopoiesis
What It Does: May limit the expansion of pro-inflammatory blood cell clones, reducing age-related vascular inflammation.
Representative Source: Huynh, 2026
6. Dose-Response Optimization
Key Players: Aerobic training volume
What It Does: Clarifies exactly "how much" exercise is needed to successfully move vascular markers, particularly in overweight and obese adults.
Representative Source: Bian et al., 2026
Practical Application: A Weekly Exercise Framework
Understanding these mechanisms is useful mainly because it lets you train with more intention. A few practical translations:
For myokine (irisin/IL-6) response: Moderate-to-vigorous aerobic activity — brisk walking, jogging, cycling, swimming — for roughly 30–60 minutes on most days appears to generate the most robust response. Shorter, higher-intensity interval sessions can produce a comparable myokine spike in less time.
For shear stress: Anything that sustainably raises heart rate and blood flow helps. Activities recruiting large muscle groups — running, rowing, cycling — tend to be most effective, though consistent daily walking (roughly 5,000–8,000 steps) meaningfully improves shear stress patterns over time.
For NLRP3 suppression: Consistency matters more than intensity here. The AMPK and mitochondrial pathways involved require repeated activation, which favors a steady weekly rhythm over occasional intense sessions.
For microRNA reprogramming: Evidence points toward aerobic and resistance training producing complementary miRNA profiles, which supports a mixed program rather than one modality alone.
Sample Weekly Template
Monday / Wednesday / Friday: 30–45 minutes moderate aerobic exercise (brisk walk, cycle, swim)
Tuesday / Thursday: 20–30 minutes resistance training (bodyweight, bands, or weights)
Saturday: 45–60 minutes recreational activity (hiking, sport, yoga)
Sunday: Rest or a gentle 15–20-minute walk
Before starting: Talk with your doctor or a cardiac rehabilitation specialist before beginning a new program, particularly if you have existing cardiovascular disease, a recent cardiac event, or significant risk factors.
Common Myths & Mistakes
Myth: "If I already take a statin, exercise doesn't add much." Statins and exercise work through largely different pathways — one primarily lowers LDL production, the other engages inflammation, endothelial function, and plaque stability. The two are complementary, not redundant.
Myth: "More intensity always means more benefit." Higher intensity can amplify certain molecular responses, but the research consistently points to consistency — repeated weekly stimulation of AMPK and mitochondrial pathways — as the stronger long-term driver of vascular benefit.
Myth: "Exercise can fully reverse plaque." Current evidence supports exercise's role in stabilizing plaque and slowing progression more clearly than it supports reversing established, calcified lesions. The larger win is preventing instability and rupture, not necessarily shrinking existing plaque.
Myth: "Walking doesn't count as 'real' cardio." Consistent daily walking measurably improves shear stress patterns and is associated with meaningful cardiovascular benefit, particularly in the 5,000–8,000 step range.
Frequently Asked Questions
How quickly does exercise start protecting my arteries? Endothelial function improvements can appear within 4–8 weeks of consistent aerobic training, with some acute anti-inflammatory effects occurring after a single session. Structural benefits like plaque stabilization build over months to years.
Is aerobic exercise better than resistance training for atherosclerosis? Both contribute, through partly different mechanisms. Aerobic training is particularly strong for irisin release, shear stress, and NLRP3 suppression; resistance training adds complementary myokine and metabolic benefits. A combined program is generally considered ideal.
Can exercise reverse existing atherosclerotic plaques? Evidence more clearly supports stabilization and slowed progression than full reversal of calcified plaque. Even so, reducing rupture risk in existing plaque meaningfully lowers cardiovascular event risk.
What is irisin, and why does it matter for heart health? Irisin is a myokine released by contracting muscle during aerobic exercise. Preclinical research links it to improved endothelial function and reduced atherosclerotic lesion formation.
I already have cardiovascular disease — is exercise safe for me? For most people with stable cardiovascular disease, supervised exercise is considered both safe and strongly beneficial, and forms the basis of standard cardiac rehabilitation programs. Work with your healthcare provider to determine appropriate intensity.
How many steps per day do I need for vascular benefits? Meaningful benefits appear to begin around 5,000–7,000 steps daily, with gains plateauing somewhat above 8,000–10,000 steps for most people. A consistent daily habit matters more than hitting an exact number.
Does sleep affect how exercise protects my arteries? Emerging research connecting sleep, exercise, and clonal hematopoiesis suggests sleep quality may influence how well exercise limits pro-inflammatory blood cell aging — an area still being actively studied.
Can diet and exercise work together on atherosclerosis? Yes — a Mediterranean-style diet and regular activity affect complementary pathways (lipid handling and gut microbiome versus shear stress, myokines, and microRNA signaling), and together represent one of the strongest non-drug approaches available.
Does exercise help even if I'm overweight or obese? Yes. Recent dose-response research specifically in adults with overweight or obesity found meaningful vascular benefits from continuous aerobic training, a population where cardiovascular risk is often elevated to begin with.
What's the difference between a stable and unstable plaque? An unstable plaque has a thin, inflamed fibrous cap prone to rupture and clot formation; a stable plaque has a thicker cap and less active inflammation. Exercise's inflammasome-related effects appear particularly relevant to improving this stability.
Conclusion & Action Steps
Atherosclerosis is often described as a cholesterol problem, but the biology tells a broader story — one of chronic inflammation, endothelial injury, and unstable plaque architecture. Exercise engages nearly every layer of that story at once: myokines calm inflammation, shear stress keeps the endothelium functional, AMPK and autophagy quiet the NLRP3 alarm system, and microRNAs slowly reshape how vascular genes behave.
None of this replaces medical therapy where it's indicated. But it does support a simple shift in how physical activity gets talked about — less as a vague suggestion, more as a specific, dosed, trackable part of cardiovascular care.
Practical next steps:
Talk with your doctor about a starting point appropriate for your current health status.
Aim for a mix of aerobic and resistance training across the week, using the template above as a starting framework.
Prioritize consistency over intensity, especially in the first 2–3 months.
Track a simple marker — steps, minutes of activity, or resting heart rate — to stay accountable.
Pair activity with a Mediterranean-style eating pattern for complementary benefit.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
Exercise and Vascular Health: How Nitric Oxide and Endothelial Function Keep Your Arteries Young
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
References
Bettariga, F., Taaffe, D. R., Galvão, D. A., Lopez, P., Bishop, C., Markarian, A. M., Natalucci, V., Kim, J.-S., & Newton, R. U. (2024). Exercise training mode effects on myokine expression in healthy adults: A systematic review with meta-analysis. Journal of Sport and Health Science, 13(6), 764–779.
Bian, J., Tan, Z., Yin, H., & Yang, J. (2026). Continuous aerobic exercise and atherosclerosis-related vascular indices in overweight and obese adults: a Bayesian three-level meta-analysis of randomized controlled trials. Frontiers in Physiology, 17, 1789752.
Hu, G., Chen, W., Zhou, X., Wang, Y., Feng, N., Gao, W., & Yu, H. (2026). Aerobic exercise stabilizes atherosclerotic plaques by suppressing miR-15a-5p-mediated repression of Semaphorin-3A in vascular smooth muscle cells. Life Sciences, 389, 124226.
Huynh, K. (2026). Sleep and exercise can limit clonal haematopoiesis clone expansion and reduce associated atherosclerosis. Nature Reviews Cardiology.
Inoue, K., Fujie, S., Uchida, M., et al. (2026). Aerobic exercise-induced irisin secretion is associated with improved endothelial function and reduced atherosclerosis in ApoE-deficient mice. Scientific Reports, 16, 12614.
Ke, S., Cao, X., Lu, X., Xu, J., Zhang, C.-Y., Xu, L., & Jiang, X. (2025). Atheroprotective roles of exercise-regulated microRNAs. Atherosclerosis, 405, 119229.
Liu, X., Hu, S., Wang, X., & Ding, Y. (2026). Exercise alleviates atherosclerosis through the modulation of the NLRP3 inflammasome. Current Molecular Medicine, 26(4), 358–375.
Yin, M. T., & Guo, L. (2025). Exercise in atherosclerosis: its beneficial effects and underlying mechanism. Frontiers in Cell and Developmental Biology, 13, 1598794.