What Should You Eat on Ozempic, Wegovy, or Mounjaro? The Complete GLP-1 Nutrition Guide to Protect Muscle and Maximize Weight Loss
Taking Ozempic, Wegovy, or Mounjaro? Discover the science-backed nutrition strategy to protect muscle, prevent deficiencies, and maximize long-term weight loss success.
NUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/5/202626 min read
What Should You Eat on GLP-1 Medications?
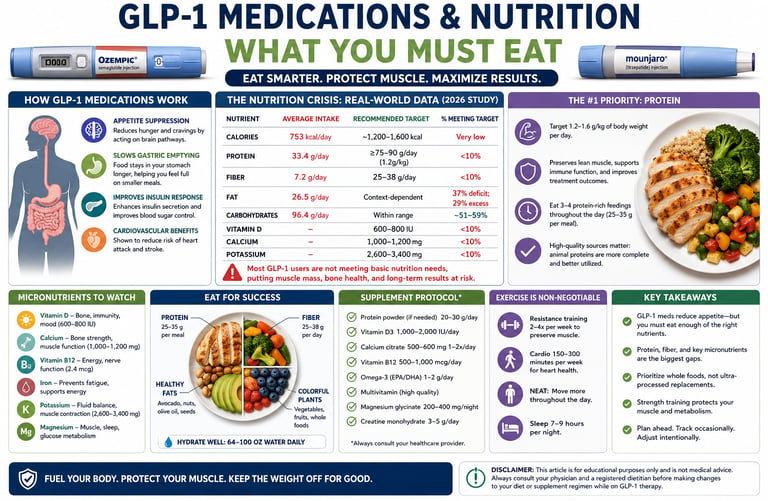
People taking Ozempic, Wegovy, Mounjaro, or other GLP-1-based medications should prioritize 1.2–1.6 g of protein per kilogram of body weight daily, consume 25–38 g of fiber, ensure adequate intake of vitamin D, calcium, potassium, magnesium, and vitamin B12, and perform regular resistance training to preserve muscle mass during weight loss. Because GLP-1 medications substantially reduce appetite, nutritional quality becomes as important as calorie reduction for maintaining long-term metabolic health.---
Key Takeaways: GLP-1 Medications & Nutrition
The GLP-1 nutrition gap is real and dangerous.
New 2026 data shows >90% of patients on Ozempic, Wegovy, Mounjaro, or Zepbound fail to meet basic protein targets. Average intake: just 753 calories and 33g protein/day. That is not sustainable weight loss — it is a pathway to muscle loss, fatigue, and rapid rebound. Ozempic Wegovy Mounjaro
Protein is your #1 job, not an afterthought.
Higher protein intake independently predicts more weight loss on GLP-1 therapy. The 2025 joint consensus from four major U.S. medical societies sets the bar at 1.2–1.6g protein per kg body weight daily. For most adults, that is 90–140g per day. Less than 10% of users hit it.
Protein quality matters: watch processed animal sources.
A surprising 2026 finding: higher proportions of animal protein were linked to less weight loss, likely due to sodium and additives in deli meats and processed foods. Prioritize legumes, tofu, Greek yogurt, eggs, fish, and lean poultry over processed meats.
Micronutrient deficiencies are nearly universal.
Fewer than 10% of GLP-1 users meet targets for vitamin D, calcium, potassium, and fiber. This mirrors bariatric surgery patients — yet GLP-1 users rarely get the same monitoring. Bone loss and sarcopenia are the hidden risks nobody talks about.
Your weekday eating is sabotaging you.
Users consume ~170 more calories, 8–9g more fat, and 370mg more sodium on weekdays vs weekends. Office lunches, takeout, and stress eating create a nutrition gap that stalls results. Meal prep is not optional.
Exercise is non-negotiable for muscle protection.
Up to 25–30% of weight lost without intervention comes from lean mass. Resistance training 2–3x per week plus 1.2–1.6g/kg protein is the minimum standard to preserve metabolism and prevent weight regain.
Supplements are not a luxury on GLP-1s.
Experts recommend discussing vitamin D3, calcium citrate, magnesium, B12, and omega-3s with your doctor. Omega-3s may specifically enhance GLP-1 efficacy and reduce muscle loss. Baseline labs at start, 3 months, and 6 months are now best practice.
Drug choice matters less than diet quality.
Tirzepatide users ate slightly more protein than semaglutide users, but drug type did not predict weight loss after adjusting for diet. Your plate drives your results more than your prescription.
Think bariatric-level nutrition support.
2026 expert perspectives argue GLP-1 therapy creates caloric restriction on par with weight-loss surgery. Patients deserve the same playbook: dietitian involvement, lab monitoring, and protein-first protocols from day one.
Introduction
If you're taking a GLP-1 medication like semaglutide (Ozempic, Wegovy) or tirzepatide (Mounjaro, Zepbound), you already know the appetite-suppressing power of these drugs is remarkable. What most people — and far too many clinicians — don't yet know is that dramatically eating less without eating smarter can quietly undermine your results, accelerate muscle loss, and set the stage for weight regain the moment you stop the medication.
Here's what the emerging science is saying: an alarming 2026 study published in the Journal of Translational Medicine found that over 90% of GLP-1 users were failing to meet basic protein targets — consuming an average of just 753 calories and 33 grams of protein per day. That's not a diet. That's a trajectory toward sarcopenic obesity, fatigue, and metabolic fragility.
This guide synthesizes the most current research — including landmark 2025–2026 consensus statements from four major U.S. medical societies — to give you the complete picture: what GLP-1 medications do to your appetite and nutritional needs, what deficiencies are putting patients at risk, and precisely how to eat to protect your muscle, maximize your weight loss, and sustain your results long-term.
You will learn:
How GLP-1 receptor agonists change your nutritional requirements
The specific protein, micronutrient, and fiber gaps the research has uncovered
Why protein source matters as much as protein amount
Practical meal planning, supplement protocols, and red flags to watch for
Answers to the questions patients and doctors are asking most right now
What GLP-1 and Dual GIP/GLP-1 Medications Actually Do
Glucagon-like peptide-1 (GLP-1) receptor agonists — including semaglutide (Ozempic, Wegovy) and liraglutide (Saxenda) — and dual GIP/GLP-1 receptor agonists like tirzepatide (Mounjaro, Zepbound) are currently the most effective pharmacological tools for managing obesity and type 2 diabetes.
They work through several simultaneous mechanisms:
Appetite suppression via the brain. These medications activate receptors in the hypothalamus and reward pathways, powerfully reducing hunger signals and cravings — particularly for high-fat, sweet, and ultra-processed foods.
Slowing gastric emptying. Food moves through your stomach more slowly, meaning you feel full longer on smaller portions.
Improved insulin sensitivity and glycemic control. The drugs enhance glucose-dependent insulin secretion, reducing blood sugar spikes.
Cardiovascular protection. Clinical trials, including the landmark SELECT trial, have shown reduced rates of heart attack and stroke in high-risk patients.
The result? Clinical trials show an average weight loss of 8–22% of body weight over 68–72 weeks, depending on the medication and adherence. That is genuinely transformative for metabolic health.
But here is the critical issue: the same mechanisms that make these drugs so effective at reducing calorie intake also mean patients often consume far too little food — and far too little of the right nutrients — to sustain lean muscle mass, support immunity, and maintain bone density during rapid weight loss.
The Hidden Nutrition Crisis Among GLP-1 Users
The most comprehensive real-world data on what GLP-1 users actually eat comes from a landmark 2026 study by Korus et al., published in the Journal of Translational Medicine. Researchers analyzed 48-hour food diaries from 387 adults (80% women; average BMI 36.4) who were actively using either a GLP-1 agonist or a dual GIP/GLP-1 agonist (tirzepatide).
The findings were striking:
Total Calories: Average intake is 753 kcal/day against a recommended target of 1,200–1,600 kcal/day. This is classified as a very low intake.
Protein: Average intake is 33.4 g/day, falling short of the recommended target of ≥75–90 g/day (based on 1.2 g/kg). The percentage meeting the target is less than 10%.
Fiber: Average intake is 7.2 g/day against a recommended target of 25–38 g/day. The percentage meeting the target is less than 10%.
Fat: Average intake is 26.5 g/day. The target is context-dependent, showing a 37% deficit or a 29% excess depending on the specific dietary framework used.
Carbohydrates: Average intake is 96.4 g/day, which falls within the target range of approximately 51–59% of total energy.
Vitamin D: Individual intake was not reported. The recommended target is 600–800 IU, and the current status shows that less than 10% meet the target.
Calcium: Individual intake was not reported. The recommended target is 1,000–1,200 mg, and the current status shows that less than 10% meet the target.
Potassium: Individual intake was not reported. The recommended target is 2,600–3,400 mg, and the current status shows less than 10% meeting
The picture that emerges is one of a carbohydrate-adequate but critically protein- and micronutrient-poor diet — a pattern that may preserve short-term energy availability while leaving the body starved of the building blocks it needs to retain muscle, support hormonal function, and maintain immune defenses.
The study concluded that dietary education emphasizing protein adequacy and micronutrient sufficiency should be a standard component of GLP-1 therapy — not an afterthought.
Notably, this finding is not isolated. A 2025 joint advisory from four major U.S. medical organizations — the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society — identified nutritional deficiency as one of the primary under-addressed risks of GLP-1 therapy, calling for structured nutritional assessment before and throughout treatment.
The Muscle Loss Problem: How Much Muscle Is Lost on GLP-1 Therapy?
One of the most important emerging concerns surrounding GLP-1 therapy is the loss of lean body mass during rapid weight reduction. Data from the STEP and SURMOUNT clinical trial programs suggest that approximately 25–40% of total weight lost may come from lean tissue, including skeletal muscle, if adequate countermeasures are not implemented.
DXA (dual-energy X-ray absorptiometry) analyses from semaglutide and tirzepatide studies consistently show reductions in both fat mass and lean mass. While some lean mass loss is expected during any weight-loss intervention, excessive muscle loss may reduce metabolic rate, impair physical function, increase frailty risk, and contribute to future weight regain.
This issue is particularly relevant in older adults and individuals with pre-existing sarcopenia. Researchers increasingly describe a phenomenon called sarcopenic obesity, where body weight decreases, but muscle quality and strength deteriorate disproportionately. A patient may appear healthier on the scale while becoming metabolically and functionally weaker.
For this reason, experts now emphasize a three-part strategy during GLP-1 therapy:
Adequate protein intake (1.2–1.6 g/kg/day)
Progressive resistance training
Monitoring of body composition rather than body weight alone
The goal is not simply to lose weight but to maximize fat loss while preserving metabolically active muscle tissue.
Why Protein Is the #1 Priority
Of all the nutritional gaps observed in GLP-1 users, inadequate protein intake carries the most serious consequences — and also represents the most powerful lever for optimizing outcomes.
What Protein Does During Weight Loss
When you lose weight — by any means — your body sheds both fat and lean muscle tissue. Without adequate protein intake, up to 25–30% of total weight lost may come from lean mass rather than fat. This matters enormously because:
Muscle is metabolically active. It burns calories at rest. Losing it lowers your resting metabolic rate, making weight maintenance harder after stopping the medication.
Muscle protects functional independence. Sarcopenia (muscle loss) increases fall risk, reduces strength, and impairs quality of life — especially in adults over 50.
Lean mass loss predicts weight regain. When the drug is stopped, patients with greater muscle loss are more likely to regain weight rapidly.
Protein and Weight Loss Efficacy
The 2026 Korus et al. study found that higher total protein intake was a significant independent predictor of greater weight loss (β = 0.446; p = 0.014) — even after controlling for drug type, treatment duration, age, and sex. This is a clinically meaningful finding: what you eat on GLP-1 therapy actively shapes how well it works for you.
How Much Protein Do You Actually Need?
The 2025 joint consensus advisory recommends:
1.2 to 1.6 grams of protein per kilogram of body weight per day during intentional weight loss on GLP-1 therapy
For a 90 kg (198 lb) person, this translates to 108–144 grams of protein per day
The average GLP-1 user in the Korus study was consuming just 33 grams — roughly one-third of the minimum target
This gap is not trivial. It represents a structural risk of sarcopenic obesity: a condition where someone loses body fat but disproportionately loses muscle, leaving them lighter but metabolically fragile and functionally weaker.
Hitting Your Protein Target: Practical Tips
Because GLP-1 medications suppress appetite so significantly, many users find it genuinely difficult to eat enough food to meet protein goals. Strategies that help:
Protein-first eating: At every meal and snack, eat your protein source before anything else
High-protein, low-volume foods: Greek yogurt, cottage cheese, egg whites, protein shakes, edamame, tofu
Smaller, more frequent meals: 4–5 smaller protein-rich meals rather than 2–3 large ones
Protein tracking apps: Use MyFitnessPal or Cronometer for at least 2–3 weeks to calibrate your intake
Liquid protein when nausea limits solid food: Whey, casein, or plant-based protein shakes can bridge gaps during GI side effects
The Animal vs. Plant Protein Debate
One of the most surprising findings from the 2026 research was the relationship between protein source and weight loss outcomes.
While higher total protein intake predicted more weight loss, a higher proportion of animal-sourced protein was actually associated with less weight loss (β = −0.517; p = 0.004). This counterintuitive finding raises important questions about food quality.
Why Might Animal Protein Underperform in This Context?
The researchers and subsequent commentators offer several hypotheses:
Processed meat problem. Many common animal protein sources — deli meats, sausages, processed chicken products — come packaged with high sodium, saturated fat, and additives associated with inflammation and water retention. The study found that higher sodium intake also independently predicted less weight loss (β ≈ −0.002; p = 0.013), suggesting that high-sodium processed animal proteins may be a double liability.
Plant proteins carry fiber and phytonutrients. Legumes, soy, and whole grains deliver protein alongside dietary fiber and anti-inflammatory compounds that may enhance gut health, satiety signals, and metabolic function.
Gut microbiome effects. Emerging research suggests that plant-based protein sources may more favorably shape the gut microbiome — which in turn influences weight regulation and GLP-1 receptor signaling itself.
What this does NOT mean: Plant protein is not inherently superior to all animal protein in every context. High-quality, minimally processed animal proteins — poultry, fish, eggs, Greek yoghurt — likely don't carry the same risks as processed meats. The finding appears to reflect food quality patterns rather than an intrinsic flaw in animal protein biology.
A Practical Protein Balance
Based on the available evidence, a balanced approach during GLP-1 therapy might include:
Prioritize: Legumes (lentils, chickpeas, black beans), tofu, tempeh, edamame, Greek yogurt, cottage cheese, eggs, fish, skinless poultry
Limit: Processed deli meats, sausages, high-sodium canned meats
Avoid conflating: A chicken breast and a hot dog are both "animal protein" — they are not equivalent in context
Critical Micronutrient Deficiencies to Watch
In the 2026 study, fewer than 10% of GLP-1 users met recommended intakes for protein, fiber, vitamin D, calcium, and potassium. This mirrors patterns seen in post-bariatric surgery patients — a population for whom micronutrient monitoring protocols are already well-established.
Vitamin D
Deficiency in vitamin D is widespread in the general population and worsened by very low calorie intake. On GLP-1 therapy, inadequate vitamin D increases risk of bone density loss, impaired immune function, muscle weakness, and mood disruption.
Target: 1,500–2,000 IU/day is often needed to maintain optimal serum levels (check your 25-OH vitamin D — target >40 ng/mL)
Calcium
With reduced food volume and often reduced dairy intake (due to nausea or food aversions), calcium shortfalls are common. Over time, calcium deficiency accelerates bone demineralization — a risk that compounds with any muscle loss from sarcopenia.
Target: 1,000–1,200 mg/day. Food sources include dairy, fortified plant milks, sardines with bones, bok choy, and almonds.
Potassium
Potassium is critical for heart rhythm, muscle contraction, and blood pressure regulation. Inadequate intake is linked to increased cardiovascular risk and muscle cramping — common complaints among GLP-1 users.
Target: 2,600–3,400 mg/day. Best food sources: avocado, sweet potato, banana, spinach, white beans.
Iron, B12, and Folate
While not specifically quantified in the Korus 2026 study, the 2025 joint advisory flags these as deficiency risks during significant caloric restriction. B12 is particularly relevant for patients avoiding animal products or who have any degree of gastric motility changes.
Fiber
Average fiber intake among GLP-1 users in the study was just 7.2 grams per day — against a recommended 25–38 grams. This is critically low. Adequate fiber is essential for:
Gut health and microbiome diversity
Glycemic control (slows glucose absorption)
Satiety (adds volume without calories)
Cardiovascular protection (lowers LDL cholesterol)
Bowel regularity (GLP-1 medications can cause constipation)
Easy fiber additions: Add chia seeds to yogurt, eat berries daily, include a serving of legumes at lunch, choose whole grains over refined carbohydrates.
Weekday vs. Weekend: Why Your Eating Pattern Matters
One of the novel findings in the 2026 Korus study was a significant and consistent difference in eating patterns between weekdays and weekends.
Participants consumed an average of 170 calories more on weekdays than at weekends (95% CI: 152–185 kcal; p < 0.001) — accompanied by higher fat intake (8–9 g more) and significantly higher sodium intake (~370 mg more).
This finding has important clinical implications:
Work environments drive higher-calorie, higher-sodium choices. Cafeteria meals, takeout lunches, office snacks, and client dinners tend to be more calorically dense and processed than home-cooked weekend meals.
Weekend eating may be healthier — or more restricted. Patients may cook more at home on weekends, or the appetite-suppressing effect of the weekly injection may coincide with the weekend for some.
Inconsistent eating patterns complicate metabolic adaptation. Regular oscillations in calorie, fat, and sodium intake between days can hinder steady weight loss progress and may contribute to the "plateaus" that frustrate many patients.
Practical Strategies to Smooth Your Weekly Pattern
Prepare weekday lunches at home and bring them in (meal prep Sunday)
Keep high-protein, low-sodium snacks at your desk (hard-boiled eggs, edamame, plain nuts, cottage cheese)
Review weekday dinner habits — restaurant meals 3–4 times a week add up significantly in sodium
Track weekday vs. weekend intake for 1–2 weeks to identify your own pattern
Monitoring Body Composition During GLP-1 Therapy
The bathroom scale cannot distinguish between fat loss and muscle loss. Monitoring body composition provides a more accurate picture of progress.
DEXA Scan
A DEXA scan is considered the gold standard for assessing:
Fat mass
Lean muscle mass
Bone mineral density
Patients undergoing substantial weight loss may benefit from baseline and follow-up DEXA assessments every 6–12 months, particularly if they are older, have osteoporosis risk factors, or are losing weight rapidly.
Bioelectrical Impedance Analysis (BIA)
Many modern smart scales estimate body fat and muscle mass using bioelectrical impedance. While less accurate than DEXA, they can help identify trends over time when measurements are taken under consistent conditions.
Waist Circumference
Waist circumference remains a simple and inexpensive marker of visceral fat reduction. A shrinking waist combined with stable strength levels generally suggests favorable body composition changes.
Grip Strength
Handgrip strength is increasingly recognized as a clinical marker of muscle function and healthy aging. Declining grip strength during GLP-1 therapy may indicate excessive loss of lean mass.
Strength Progression
Perhaps the most practical measure is gym performance. If strength in exercises such as squats, rows, presses, or deadlifts is maintained or improving, muscle preservation is more likely. Rapid strength decline despite weight loss should prompt reassessment of protein intake and training habits.
What the Experts Recommend: 2025–2026 Consensus Guidelines
In 2025, four of the most authoritative bodies in obesity and nutrition medicine jointly published landmark guidance: the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society. Published in the journal Obesity, this advisory outlines eight nutritional priorities for patients on GLP-1 therapy.
The Eight Nutritional Priorities
1. Patient-centered initiation. Use a shared decision-making framework (the "5 A's": Assess, Advise, Agree, Assist, Arrange) to align treatment with the patient's goals, lifestyle, and social context.
2. Baseline nutrition assessment. Every patient starting GLP-1 therapy should receive a validated nutritional screening and comprehensive assessment — including dietary history, food preferences, cultural practices, weight history, and any conditions affecting nutrient absorption.
3. GI side effect management. Nausea, vomiting, constipation, and diarrhea are common, especially during dose escalation. Strategies include gradual dose titration, smaller more frequent meals, adequate hydration, and temporarily reducing high-fat or high-fiber foods early in treatment.
4. Dietary preference navigation. GLP-1 medications can alter food preferences and lead to aversions to previously enjoyed foods. Nutrition counseling should address maintaining adequate intake despite these changes.
5. Micronutrient deficiency prevention. A diet rich in fruits, vegetables, whole grains, lean proteins, and healthy fats is the foundation. Supplementation with vitamin D, calcium, B12, iron, and folate should be considered, with regular monitoring of blood levels.
6. Muscle and bone preservation. Consume 1.2–1.6 g protein/kg/day. Combine with resistance training at least 2–3 times per week. Consider bioelectrical impedance analysis or DEXA scans to monitor lean mass.
7. Maximizing weight loss efficacy. Pair pharmacotherapy with structured nutrition and physical activity counseling. Trials show that medication combined with intensive lifestyle intervention produces greater and more sustained weight loss than medication alone.
8. Supportive lifestyle measures. Address sleep quality, stress management, alcohol use, and social support. Screen for depression and binge eating disorder, which are prevalent in obesity populations and can undermine adherence.
Lessons from Bariatric Surgery
A 2026 perspective paper published in the International Journal of Obesity by Spreckley, Ruggiero, and Brown draws a critical parallel: GLP-1 therapy produces caloric restriction and weight loss at a magnitude comparable to bariatric surgery — yet without the robust post-operative nutritional monitoring protocols that surgery patients routinely receive.
Bariatric surgery patients are typically enrolled in:
Pre-operative nutritional assessment and education
Post-operative supplementation protocols (multivitamin, calcium citrate, vitamin D, B12, iron)
Regular lab work at 3, 6, and 12 months post-surgery
Long-term follow-up with a dietitian
GLP-1 users, by contrast, often receive a prescription with minimal dietary guidance.
The authors argue that the magnitude of metabolic change on GLP-1 therapy warrants bariatric-level nutritional support — including routine lab monitoring, individualized supplementation, and dietitian involvement from day one.
This "nutrition guidance gap" is one of the most important structural challenges in current obesity pharmacotherapy.
GLP-1 vs. Dual GIP/GLP-1: Do Nutrition Needs Differ?
The 2026 Korus study also compared dietary patterns between patients using GLP-1 agonists alone (semaglutide, liraglutide, dulaglutide) versus those on the dual GIP/GLP-1 agonist tirzepatide.
Key findings:
Tirzepatide users consumed 4.3 g/day more total protein and 5.4 g/day more animal protein than GLP-1 users
Tirzepatide users consumed ~16 g/day fewer carbohydrates and slightly less fiber
No significant differences were found in fat or sodium intake
Importantly, despite these differences in macronutrient profiles, the type of medication did not independently predict weight loss outcomes after adjusting for treatment duration and dietary factors. This suggests that how you eat on either medication matters more than which medication you're taking.
Both drug classes share the same fundamental nutritional risks — inadequate protein, micronutrient deficiencies, low fiber — and both populations benefit from the same nutritional strategies.
Your Complete GLP-1 Nutrition Meal Plan Framework
Based on the 2025–2026 evidence, here is a practical framework for optimizing nutrition during GLP-1 or dual GIP/GLP-1 therapy. This is not a rigid meal plan but a flexible structure you can customize with your dietitian.
Daily Nutrition Targets (General Guidance)
The Protein/Fiber Combo: A great rule of thumb is to aim for 25–30g of protein and 8–10g of fiber per main meal. For example, a morning bowl of Greek yogurt topped with a cup of raspberries and two tablespoons of chia seeds instantly knocks out about 25g of protein and 13g of fiber.
The Calcium/Vitamin D Tag Team: Calcium needs Vitamin D to be properly absorbed in your gut. If you end up taking a calcium supplement to bridge a gap, try to split it into doses of 500 mg or less (your body struggles to absorb more than that at one time) and take it with food.
The Sodium/Potassium Balance: Think of these two as a see-saw. While lowering sodium is great, increasing your potassium from whole foods (like avocados, leafy greens, and potatoes) actually helps your body flush out excess sodium and relaxes blood vessels.
Sample Day Structure (Protein-First Approach)
Breakfast (aim for 25–35 g protein)
Greek yogurt (plain, 2%) with berries and chia seeds
2 scrambled eggs
Small handful of walnuts
Lunch (aim for 30–40 g protein)
Large salad with grilled chicken or salmon, chickpeas, olive oil, lemon
Whole grain wrap or side of quinoa (if tolerated)
Afternoon Snack (aim for 15–20 g protein)
Cottage cheese with sliced cucumber
OR: Edamame with a sprinkle of sea salt
OR: Protein shake (plant-based or whey)
Dinner (aim for 30–40 g protein)
Lentil and vegetable soup with tofu
OR: Baked fish with roasted vegetables and sweet potato
Small side salad with olive oil
Evening (optional, if still under protein goal)
Casein protein shake or a small bowl of cottage cheese
Note: Many GLP-1 users cannot eat large volumes at any single sitting. Distribute protein across 4–5 smaller eating occasions rather than relying on 3 large meals.
Foods to Emphasize
Protein sources: Greek yogurt, cottage cheese, eggs, tofu, tempeh, edamame, lentils, chickpeas, fish (salmon, tuna, sardines), skinless chicken breast, turkey
Fiber sources: Leafy greens, broccoli, chia seeds, flaxseed, berries, apples, avocado, oats, legumes
Healthy fats: Olive oil, avocado, nuts, seeds, fatty fish
Nutrient-dense carbohydrates: Sweet potato, quinoa, brown rice, oats, whole grain bread
Foods to Limit
Processed and deli meats (high sodium + saturated fat)
Ultra-processed snack foods
Sugary beverages and juices
Fried foods (worsen GI side effects and are high in empty calories)
High-sodium restaurant meals as a daily habit
Supplement Protocol for GLP-1 Users
Based on the expert consensus and the nutritional deficiency data, the following supplements warrant consideration. Always confirm specific dosing and need with your healthcare provider through blood testing.
Core Supplements to Discuss with Your Doctor
Morning (With Breakfast / Empty Stomach)
Vitamin B12 (500–1,000 mcg)
How: Sublingual (under the tongue) or methylcobalamin on an empty stomach.
Why: Vital for nerve function and red blood cell production, which can drop during calorie restriction.
Vitamin D3 + K2 (1,500–2,000 IU D3)
How: Take with breakfast (requires dietary fat for absorption).
Why: D3 pulls calcium from your gut into your blood; K2 acts as the traffic cop, driving that calcium directly into your bones instead of your arteries.
Probiotics (Multi-strain Lactobacillus/Bifidobacterium)
How: 30 minutes before your first meal or right as you eat.
Why: Mitigates GI stress and protects your gut microbiome during shifts in food volume or composition.
Mid-Day & Evening (With Meals)
Calcium Citrate (500 mg — Dose 1 of 2)
How: Take with lunch.
Why: Protects bone mineral density. The citrate form absorbs easily without needing heavy stomach acid, preventing bloating.
Omega-3 EPA/DHA (2–4 g combined)
How: Take with your largest, highest-fat meal of the day.
Why: Acts as a powerful anti-inflammatory and actively helps preserve lean muscle mass during weight loss.
Calcium Citrate (500 mg — Dose 2 of 2)
How: Take with dinner.
Why: Splitting your calcium is critical—your body cannot efficiently absorb more than 500 mg at one time.
Anytime / Bedtime
Collagen Peptides (15–20 g)
How: Mix into liquid anytime (pre- or post-workout is ideal).
Why: Supplies glycine and proline to support joint and connective tissue recovery. (Note: Count the calories, but do not count this toward your daily complete protein target).
Magnesium Glycinate (200–400 mg)
How: Take 30–60 minutes before bed.
Why: The glycinate form crosses into the brain easily to calm the nervous system, relax sore muscles, improve sleep quality, and gently prevent constipation.
A 2025 narrative review in Obesities by Dias et al. specifically highlighted that omega-3 polyunsaturated fatty acids may enhance GLP-1 analogue efficacy, attenuate lean mass loss via anti-inflammatory pathways, and complement the drug's metabolic effects. Probiotics and prebiotics were also identified as potentially reducing GI intolerability — one of the leading reasons patients discontinue therapy.
⚠️ Do not self-prescribe high-dose supplements. Excess calcium, iron, and vitamin D each carry risks. Get baseline labs and follow up at 3 and 6 months.
Exercise: The Non-Negotiable Complement
No nutrition strategy is complete without addressing physical activity — particularly resistance training.
During GLP-1-assisted weight loss, exercise performs three critical functions:
Preserves lean muscle mass. Resistance training provides the anabolic stimulus that signals the body to retain — and potentially build — muscle tissue even during caloric restriction.
Enhances the drug's metabolic effects. Combining GLP-1 therapy with structured physical activity counseling produces greater and more sustained weight loss than medication alone.
Protects bone density. Weight-bearing and resistance exercise stimulate bone remodeling, counteracting the bone mineral loss risk that accompanies rapid weight reduction.
Minimum Recommended Activity
Resistance training: 2–3 sessions per week, targeting all major muscle groups (legs, back, chest, shoulders, arms). This can be bodyweight, bands, dumbbells, or machines.
Aerobic activity: 150–300 minutes per week of moderate intensity (brisk walking, cycling, swimming)
Daily movement: Aim for 7,000–10,000 steps per day; prolonged sitting worsens metabolic outcomes
For patients new to exercise, a brief consultation with a physical therapist or certified trainer can make the difference between consistent adherence and injury-related dropout.
Common Myths & Mistakes
Myth 1: "The medication does the work — I just need to eat less"
Reality: The medication creates the opportunity by reducing appetite. Without adequate protein and nutrient intake, you risk losing muscle instead of fat, undermining long-term results.
Myth 2: "I'm not hungry, so I don't need to eat as much protein"
Reality: Your body's protein requirement is determined by your muscle mass and metabolic needs — not your hunger level. The drug suppresses appetite signals, but your tissues still need protein to maintain function.
Myth 3: "Plant-based proteins are always better"
Reality: The research suggests that high-sodium, processed animal proteins (like deli meats) are associated with worse outcomes — not all animal proteins. High-quality unprocessed animal proteins (eggs, fish, Greek yogurt) remain excellent choices.
Myth 4: "I don't need supplements if I eat well"
Reality: Given that the average GLP-1 user is consuming only ~750 calories per day, meeting all micronutrient needs from food alone is extremely difficult. Targeted supplementation guided by blood work is appropriate for most patients.
Myth 5: "Tirzepatide is more effective than semaglutide, so nutrition matters less"
Reality: The 2026 data found no significant difference in weight loss outcomes based on drug type after controlling for dietary factors. Both medications carry the same nutritional risks. What you eat matters equally on either drug.
Myth 6: "I can go back to eating normally after I stop the medication"
Reality: The greatest risk of GLP-1 therapy is weight regain upon discontinuation. Muscle preservation through adequate protein and resistance exercise during treatment is the single best insurance policy against rapid rebound.
Mistake: Ignoring GI side effects rather than managing them nutritionally
GI symptoms — nausea, vomiting, constipation, gastroparesis — are real barriers to adequate nutrition. They should be proactively managed with gradual dose titration, smaller meals, ginger tea, adequate hydration, and dietary adjustment (temporarily lower fat and fiber during flares), not simply tolerated.
Evidence Summary Table
Lean Mass Loss & Nutritional Risks
Up to 30% of weight lost can be muscle: A 2024 review (Neeland et al.) notes that without specific intervention strategies, 25% to 30% of total weight loss on GLP-1 therapy can come from lean mass rather than fat.
Severe protein deficiencies are widespread: A 2026 retrospective cohort study of 387 patients (Korus et al.) revealed that fewer than 10% of GLP-1 users met their protein targets, with an alarmingly low average intake of just 33g of protein per day.
A massive medical guidance gap exists: A recent perspective review (Spreckley et al.) highlighted a critical shortfall in patient care, arguing that GLP-1 therapy actually requires bariatric-level nutritional monitoring that patients are currently not receiving.
Consensus Guidelines & Targets
Clinical consensus sets a 1.2–1.6 g/kg protein target: A 2025 consensus advisory representing four major U.S. medical societies (Mozaffarian et al.) established 8 absolute nutritional priorities for GLP-1 patients, specifically mandating a protein target of 1.2 to 1.6 grams per kilogram of body weight daily.
Higher protein actually predicts better weight loss: Beyond just protecting muscle, the 2026 cohort data (Korus et al.) showed that patients who consumed higher total protein achieved significantly greater overall weight loss.
Therapy Efficacy, Scale, & Optimization
Targeted supplements may boost medication efficacy: A 2025 literature synthesis (Dias et al.) found that supplementing with high-quality protein, Omega-3 fatty acids, and probiotics can actively enhance GLP-1 medication efficacy while mitigating common gastrointestinal side effects.
Massive global scale and adherence issues: A 2025 observational study (Rodriguez et al.) estimates that 9 to 12 million people globally are now utilizing GLP-1 therapies, though long-term patient discontinuation patterns remain a major area of study.
Long-term safety and cardiovascular benefits are proven: The landmark SELECT clinical trial (Ryan et al., 2024), which tracked 17,604 patients in a randomized controlled trial, robustly confirmed the long-term weight loss and protective cardiovascular benefits of semaglutide.
FAQs
How much protein should I eat on Ozempic or Wegovy?
The 2025 expert consensus recommends 1.2 to 1.6 grams of protein per kilogram of body weight per day during GLP-1 therapy. For a 180-lb (82 kg) person, that's approximately 98–131 grams of protein per day. Most patients on GLP-1 medications are consuming far less — averaging around 33 grams in one 2026 study — which puts them at risk for significant muscle loss.
Can GLP-1 medications cause muscle loss?
Yes. Research published in Diabetes, Obesity and Metabolism (2024) found that without adequate protein and resistance exercise, up to 25–30% of weight lost on GLP-1 therapy may come from lean muscle rather than fat. This underscores the importance of protein-first eating and strength training throughout treatment.
What vitamins and supplements should I take on semaglutide or tirzepatide?
The most commonly recommended supplements include vitamin D3, calcium citrate, magnesium, vitamin B12, and omega-3 fatty acids. A 2025 review found evidence that omega-3s may specifically enhance GLP-1 medication efficacy and reduce muscle loss. However, your exact supplement needs should be guided by blood work, not generic recommendations.
Why do I feel worse on weekdays while taking GLP-1 medications?
A 2026 study found that GLP-1 users consumed significantly more calories, fat, and sodium on weekdays than weekends — likely due to workplace food environments, stress eating, and social eating patterns. Higher weekday sodium and fat intake was associated with less optimal weight loss outcomes. Meal prepping and intentional weekday food choices can help close this gap.
Is plant-based protein better than animal protein on GLP-1 therapy?
Not categorically. The research found that a higher proportion of animal-sourced protein was linked to slightly worse weight loss outcomes — but this appears to reflect the fact that many common animal protein sources (deli meats, processed foods) come packaged with high sodium and saturated fat. High-quality, minimally processed animal proteins like eggs, fish, and Greek yogurt remain excellent choices. A balance of plant and animal sources is likely optimal.
Should I eat if I'm not hungry on GLP-1 medications?
This is one of the most important questions in GLP-1 nutritional management. The short answer is: yes, you need to eat purposefully even when not hungry, because your body's protein and micronutrient requirements do not disappear with your appetite. Skipping meals entirely — especially protein-rich ones — accelerates muscle loss and nutritional deficiency. Work with a dietitian to establish a regular eating schedule with protein targets at each occasion.
How do I manage nausea on semaglutide or tirzepatide?
GI side effects are most pronounced during dose escalation. Evidence-based strategies include eating smaller, more frequent meals; avoiding high-fat, greasy, and heavily spiced foods; staying well hydrated; ginger tea or ginger chews; eating slowly and not lying down immediately after meals; and temporarily reducing dietary fiber until symptoms improve. If nausea is severely limiting your nutrition, speak to your prescriber — dose titration can be slowed.
Will I gain the weight back when I stop GLP-1 medication?
Clinical data show that weight regain after stopping GLP-1 therapy is common, largely because the underlying biological drivers of obesity (altered satiety signaling, metabolic adaptation) return when the drug is discontinued. However, patients who have preserved more lean muscle mass during treatment tend to have a better metabolic foundation for weight maintenance. This makes adequate protein intake and resistance training during therapy a form of long-term insurance — not just a short-term strategy.
Do GLP-1 medications interact with any nutritional supplements?
No major drug-nutrient interactions have been identified for commonly recommended supplements. However, high-dose iron supplements can worsen GI side effects. Some supplements (especially high-dose calcium) should be taken separately from medication doses. Always disclose all supplements to your prescriber.
How long does it take for GLP-1 medications to work?
The 2026 Korus research confirmed that treatment duration is the single strongest predictor of weight loss — each additional week of therapy was associated with approximately 0.73 kg greater weight reduction. This means patience is essential: maximum benefits typically emerge at 52–72 weeks. Nutrition optimization amplifies these long-term outcomes.
Action Steps & Conclusion
GLP-1 and dual GIP/GLP-1 receptor agonists represent a genuine turning point in obesity medicine. For millions of people, these medications are enabling a degree of weight loss and metabolic improvement that was previously out of reach. But the science is now clear: the medication alone is not enough.
The emerging research from 2025–2026 reveals that most GLP-1 users are walking a nutritional tightrope — eating too little, too poorly, and without the professional support needed to protect their muscle mass, bone density, and long-term metabolic health.
The good news is that the gaps are entirely addressable — with knowledge, intention, and the right support.
Your Action Checklist
[ ] Request a baseline nutrition assessment before or immediately after starting GLP-1 therapy. Ask for blood work that includes vitamin D (25-OH), B12, iron/ferritin, magnesium, calcium, and a complete metabolic panel.
[ ] Calculate your protein target: Multiply your current weight in kg by 1.2 and 1.6 to find your daily protein range. Write it down and track it for at least two weeks.
[ ] Adopt protein-first eating: Protein before anything else at every meal and snack.
[ ] Identify your top 5 high-protein foods that you can tolerate well and keep them stocked at all times.
[ ] Start resistance training: Even 2 sessions per week of 20–30 minutes makes a significant difference in lean mass preservation.
[ ] Review your weekday food environment: What are you eating Monday–Friday for lunch? Are there high-sodium, processed options dominating? Meal prep is your best tool here.
[ ] Discuss supplementation with your prescriber — at minimum, vitamin D and calcium deserve evaluation.
[ ] Schedule a follow-up at 3 months and 6 months for nutritional labs and body composition assessment if available.
[ ] Work with a registered dietitian experienced in obesity or bariatric nutrition. This is the single highest-leverage investment you can make alongside your medication.
The medications open the door. What you eat determines whether you walk through it into lasting health — or find yourself cycling back in a few years. Feed the outcome you want.
Medical Disclaimer: This article is for educational purposes. Always work with your prescribing physician and a registered dietitian before making significant changes to your diet or supplement regimen while on GLP-1 therapy.
Explore related reads
Can GLP-1 Drugs Prevent Heart Attacks? New Trial Data Changes Everything
References
Abbott Nutrition Health Institute. (2025). Nutritional priorities to support GLP-1 therapy for obesity [Transcript]. ANHI Nutrition Research Reviews. http://anhi.org
Coelho-Junior, H. J., Calvani, R., Azzolino, D., Marzetti, E., & Landi, F. (2022). Protein intake and sarcopenia in older adults: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 19(14), Article 8718. https://doi.org/10.3390/ijerph19148718
Dias, D. D., Vasconcelos, R. A., Souza, A. C. R., Menezes, C., Silva, I. S. T., & Name, J. J. (2025). Nutritional approaches to enhance GLP-1 analogue therapy in obesity: A narrative review. Obesities, 5(4), 88. https://doi.org/10.3390/obesities5040088
Drucker, D. J. (2024). Efficacy and safety of GLP-1 medicines for type 2 diabetes and obesity. Diabetes Care, 47(11), 1873–1888. https://doi.org/10.2337/dci24-0003
Hou, V., & Madden, K. (2022). Assessing the effects of dietary protein supplementation on sarcopenia in community-dwelling older adults. Canadian Geriatrics Journal, 25(4), 390–403.
Iqbal, J., Wu, H. X., Hu, N., & et al. (2022). Effect of GLP-1 receptor agonists on body weight in adults with obesity without diabetes: A systematic review and meta-analysis of randomized control trials. Obesity Reviews, 23(6), Article e13435. https://doi.org/10.1111/obr.13435
Korus, S., Cembrowska-Lech, D., Kłoda, K., & et al. (2026). Dietary intake patterns and nutritional adequacy among adults with overweight or obesity treated with GLP-1 or dual GIP/GLP-1 receptor agonists — preliminary study. Journal of Translational Medicine, 24, Article 532. https://doi.org/10.1186/s12967-026-07702-4
Lin, F., Yu, B., Ling, B., & et al. (2023). Weight loss efficiency and safety of tirzepatide: A systematic review. PLoS ONE, 18(5), Article e0285197. https://doi.org/10.1371/journal.pone.0285197
Mozaffarian, D., Agarwal, M., Aggarwal, M., & et al. (2025). Nutritional priorities to support GLP-1 therapy for obesity: A joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society. Obesity, 33(8), 1475–1503. https://doi.org/10.1002/oby.24336
Neeland, I. J., Linge, J., & Birkenfeld, A. L. (2024). Changes in lean body mass with glucagon-like peptide-1-based therapies and mitigation strategies. Diabetes, Obesity and Metabolism, 26(Suppl 4), 16–27. https://doi.org/10.1111/dom.15728
Perez-Montes De Oca, A., Pellitero, S., & Puig-Domingo, M. (2021). Obesity and GLP-1. Minerva Endocrinologica, 46(2), 168–176. https://doi.org/10.23736/S2724-6507.20.03359-5
Prokopidis, K., Daly, R. M., & Suetta, C. (2025). Weighing the risk of GLP-1 treatment in older adults: Should we be concerned about sarcopenic obesity? The Journal of Nutrition, Health & Aging, 29(10), Article 100652. https://doi.org/10.1016/j.jnha.2025.100652
Rodriguez, P. J., Zhang, V., Gratzl, S., & et al. (2025). Discontinuation and reinitiation of dual-labeled GLP-1 receptor agonists among US adults with overweight or obesity. JAMA Network Open, 8(1), Article e2457349. https://doi.org/10.1001/jamanetworkopen.2457349
Ryan, Disna H., Lingvay, I., Deanfield, J., & et al. (2024). Long-term weight loss effects of semaglutide in obesity without diabetes in the SELECT trial. Nature Medicine, 30(7), 2049–2057. https://doi.org/10.1038/s41591-024-02996-7
Scheen, A. J. (2023). Dual GIP/GLP-1 receptor agonists: New advances for treating type-2 diabetes. Annales d'Endocrinologie, 84(2), 316–321. https://doi.org/10.1016/j.ando.2023.03.001
Spreckley, M., Ruggiero, C. F., & Brown, A. (2026). Bridging the nutrition guidance gap for GLP-1 receptor agonist therapy assisted weight loss: Lessons from bariatric surgery. International Journal of Obesity, 50, 265–267. https://doi.org/10.1038/s41366-025-01952-w
van Bloemendaal, L., Veltman, D. J., Ten Kulve, J. S., & et al. (2015). Brain reward-system activation in response to anticipation and consumption of palatable food is altered by GLP-1 receptor activation in humans. Diabetes, Obesity and Metabolism, 17(9), 878–886. https://doi.org/10.1111/dom.12506
Waters, D. L., Aguirre, L., Gurney, B., Sinacore, D. R., Qualls, C., & Villareal, D. T. (2022). Effect of aerobic or resistance exercise, or both, on intermuscular and visceral fat and physical and metabolic function in older adults with obesity while dieting. The Journals of Gerontology: Series A, 77(1), 131–139. https://doi.org/10.1093/gerona/glab146