Sarcopenia vs. Osteoporosis: Key Differences for Bone & Muscle Health
Learn the difference between osteoporosis and Sarcopenia, how they combine as osteosarcopenia, and the best evidence-based strategies to prevent fractures, muscle loss, frailty, and disability after age 50.
SARCOPENIA
DR T S DIDWAL MD
5/20/202617 min read
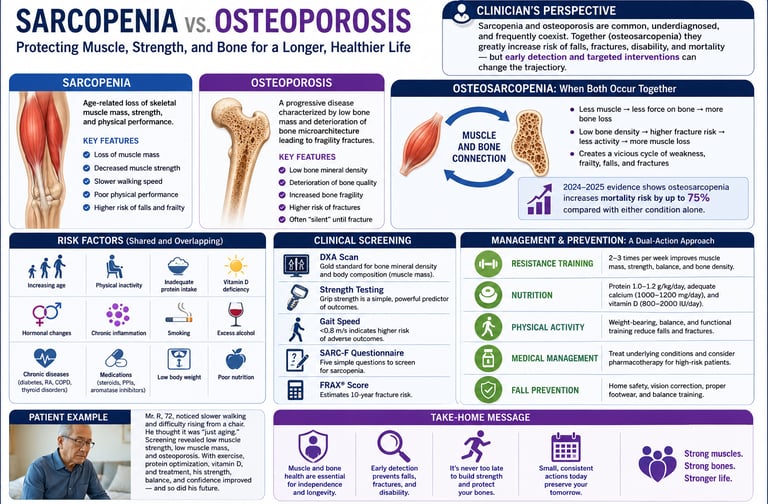
Sarcopenia and osteoporosis are age-related conditions that weaken muscles and bones, increasing the risk of falls, fractures, frailty, and loss of independence. When both occur together — called osteosarcopenia — mortality risk rises significantly. Resistance training, adequate protein, vitamin D, and early screening are key strategies for prevention and healthy aging.
After the age of 50, many people begin noticing subtle physical changes they instinctively dismiss as “normal aging.” Climbing stairs feels harder. Carrying groceries becomes unexpectedly tiring. Balance feels less stable. A once-powerful handshake weakens. Then, sometimes without warning, a minor fall leads to a devastating fracture that permanently changes independence, mobility, and quality of life. What most adults do not realize is that two silent biological conditions may already be progressing beneath the surface: Sarcopenia and osteoporosis.
For decades, muscle loss and bone loss were treated as separate consequences of aging. Modern science now shows they are deeply interconnected disorders that frequently develop together, reinforcing one another in a destructive cycle of weakness, frailty, falls, fractures, and disability (Chen et al., 2024; Liu et al., 2025). Sarcopenia progressively reduces muscle strength, balance, and mobility, while osteoporosis silently weakens bone structure until even a small stumble can cause catastrophic injury. Together, they form a dangerous syndrome increasingly known as osteosarcopenia — one of the fastest-growing but most underrecognized threats to healthy aging.
Emerging 2024–2025 research suggests the consequences extend far beyond mobility alone. Older adults with both conditions face significantly higher risks of hospitalization, loss of independence, institutionalization, and premature death (Jin et al., 2025; Liu et al., 2025). Yet there is also encouraging news: unlike many aspects of aging once thought inevitable, muscle and bone decline are highly modifiable. Exercise, nutrition, early screening, and resistance training can meaningfully slow — and sometimes partially reverse — this trajectory. The earlier the intervention begins, the greater the opportunity to preserve strength, resilience, and long-term healthspan.
Key Takeaways About Sarcopenia and Osteoporosis
1. Muscle Loss and Bone Loss Often Occur Together
Modern aging research shows that Sarcopenia and osteoporosis are biologically connected conditions that frequently coexist as osteosarcopenia, dramatically increasing the risk of frailty, falls, fractures, and disability.
2. Osteosarcopenia Can Increase Mortality by Up to 75%
Recent large-scale studies show that adults with both sarcopenia and osteoporosis face substantially higher risks of hospitalization, loss of independence, fractures, and premature death compared with either condition alone.
3. Osteoporosis Is Often Silent Until a Fracture Occurs
Bone loss usually develops without symptoms for years. Many people first discover osteoporosis only after a hip, spine, or wrist fracture caused by a minor fall or routine movement.
4. Sarcopenia Begins Earlier Than Most People Realize
Age-related muscle decline can start as early as the fourth decade of life and accelerates after age 50, leading to weakness, slower walking speed, impaired balance, and reduced physical resilience.
5. Resistance Training Is the Most Powerful Dual Therapy
Progressive strength training improves muscle mass, balance, mobility, and bone density simultaneously, making it one of the most evidence-based interventions for healthy aging and fall prevention.
6. Protein, Vitamin D, and Metabolic Health Matter
Adequate dietary protein, vitamin D optimization, healthy body composition, and physical activity are essential for preserving musculoskeletal health and reducing age-related decline.
Early Screening Can Protect Long-Term Independence
DXA scans, grip strength testing, gait-speed assessment, FRAX® scoring, and SARC-F screening help identify high-risk adults before irreversible weakness, fractures, and frailty develop.
Understanding Osteoporosis: When Bones Become Brittle
Osteoporosis is a chronic skeletal disorder in which bone mineral density (BMD) falls so low that bones become porous and fracture-prone. It is defined clinically by a T-score of –2.5 or lower on a dual-energy X-ray absorptiometry (DXA) scan, which compares your bone density to that of a healthy young adult.
Often called the "silent disease," osteoporosis produces no pain, no visible symptoms, and no warning signs — until a bone breaks. The most common fracture sites are the hip, the vertebrae of the spine, and the wrist. A hip fracture in an older adult is not merely an inconvenience; it is a life-altering event associated with a dramatically increased risk of disability, institutionalization, and death within the following year.
How Bone Loss Happens
Bone is living tissue. Throughout your life, old bone is continuously broken down by cells called osteoclasts, while new bone is formed by osteoblasts. In youth, formation outpaces resorption, building bone density that peaks in your late 20s to early 30s. After that, the balance begins to shift — and in women, the decline accelerates sharply after menopause, when falling estrogen levels remove a key brake on osteoclast activity.
Other risk factors include long-term use of corticosteroids, chronic conditions such as rheumatoid arthritis or hyperthyroidism, low dietary calcium and vitamin D, physical inactivity, smoking, and excessive alcohol consumption.
Global burden: Osteoporosis affects over 200 million people worldwide, predominantly postmenopausal women and elderly men, though no demographic is entirely immune.
Understanding Sarcopenia: When Muscles Waste Away
Sarcopenia — a term coined in 1989 from the Greek words for "poverty of flesh" — refers to the progressive, age-related loss of skeletal muscle mass, strength, and physical performance. Unlike osteoporosis, sarcopenia does not stay silent. Its hallmarks are visible: weakness when gripping objects, difficulty rising from a chair, a slower walking pace, and a growing reluctance to attempt physical tasks that once felt routine.
According to the revised European consensus criteria (EWGSOP2), diagnosis requires evidence of low muscle strength combined with low muscle mass and/or low physical performance (Cruz-Jentoft et al., 2019). This three-component model reflects the understanding that sarcopenia is not merely about size — it is fundamentally about function.
Who Is Affected?
Sarcopenia affects 5–13% of adults in their 70s, rising to 11–50% by age 80, depending on the population studied. Projections suggest that by 2050, over 500 million older adults worldwide will be living with sarcopenia. It is not merely a problem of vanity or athletic performance — sarcopenia predicts falls, hospitalization, frailty, and premature death.
Why Muscle Disappears With Age
Several converging biological mechanisms drive sarcopenia:
Hormonal decline: Testosterone, estrogen, growth hormone, and insulin-like growth factor-1 (IGF-1) all promote muscle protein synthesis. Their age-related decline tips the balance toward muscle catabolism.
Chronic low-grade inflammation ("inflammaging"): Elevated inflammatory cytokines — particularly interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) — directly impair muscle cell regeneration and accelerate protein breakdown.
Mitochondrial dysfunction: Aging muscle cells become less efficient at energy production, reducing their capacity to sustain physical activity and recover from exertion.
Neuromuscular changes: The motor neurons that signal muscle fibers to contract become less efficient with age, causing the selective loss of fast-twitch (type II) muscle fibers responsible for power and speed.
Inadequate protein intake: Many older adults consume insufficient dietary protein to support muscle protein synthesis, worsening the imbalance between muscle building and breakdown.
Sarcopenia vs. Osteoporosis: The Critical Differences
While sarcopenia and osteoporosis share risk factors and often coexist, they are fundamentally distinct conditions affecting different biological systems. Understanding those differences is the first step toward appropriate screening and management.
Osteoporosis
System affected: Skeletal system (bones)
Primary symptom: Usually silent until a fracture occurs
Main health risk: Hip, spine, and wrist fractures
Main diagnostic tool: DXA scan showing T-score ≤ 2.5
Screening tool: FRAX® fracture-risk calculator
Most affected population: Primarily postmenopausal women
Primary medications: Bisphosphonates, denosumab, anabolic bone therapies
Core lifestyle treatment: Weight-bearing exercise, calcium, and vitamin D
Sarcopenia
System affected: Musculoskeletal system (skeletal muscle)
Primary symptom: Weakness, slower walking speed, fatigue
Main health risk: Falls, frailty, mobility loss, disability
Main diagnostic tools: Grip-strength testing, DXA/BIA muscle-mass assessment, gait-speed testing
Screening tool: SARC-F questionnaire
Most affected population: Adults over 70, both men and women
Primary medications: No approved drug therapy currently exists
Core lifestyle treatment: Progressive resistance training and adequate dietary protein intake.
A critical point highlighted by Zhan et al. (2025) in Scientific Reports is that different diagnostic criteria for sarcopenia yield different predictive values for osteoporosis and fracture risk. This means that how sarcopenia is defined and measured directly affects which patients are identified as high-risk — underscoring the importance of using validated, standardized assessment tools in clinical practice.
When Both Strike Together: The Dangerous World of Osteosarcopenia
When osteoporosis and sarcopenia coexist in the same individual, clinicians now recognize a distinct and far more dangerous clinical entity: osteosarcopenia. A comprehensive meta-analysis and systematic review by Chen et al. (2024), encompassing data from over 64,000 individuals, revealed that osteosarcopenia affects approximately 18% of older adults globally — and the consequences are severe:
54% increased risk of falls
Doubled risk of fractures
75% higher mortality rates
These figures are not merely additive — they reflect genuine biological synergy. Muscle loss reduces the mechanical loading that bones need to stimulate new bone formation. Weaker bones increase fracture risk when falls occur. Fractures lead to immobilization, which causes further muscle loss. The cycle compounds itself relentlessly.
The 2025 cohort study by Liu et al. confirmed these findings in a U.S. population, demonstrating that the additive effect of sarcopenia and osteoporosis on all-cause mortality is clinically significant and independent of other confounding factors — making osteosarcopenia one of the most pressing yet underaddressed conditions in geriatric medicine today.
Geographic and Gender Variations
Research by Jin et al. (2025) found striking variations in osteosarcopenia risk by geography and sex:
European populations face a 4.37 times higher osteoporosis risk when sarcopenia is present
Asian populations face a 2.66 times higher risk
American populations face a 2.32 times higher risk
Males with sarcopenia carry 4.74 times higher osteoporosis risk, compared to 3.46 times in females
These variations likely reflect differences in body composition norms, dietary patterns, physical activity levels, and the diagnostic criteria used across different healthcare systems.
Diagnosis: How Each Condition Is Identified
Diagnosing Osteoporosis
The cornerstone of osteoporosis diagnosis is the DXA scan, which measures bone mineral density at the hip, lumbar spine, and sometimes forearm, generating a T-score. Screening is recommended for:
All women aged 65 and older
Postmenopausal women under 65 with risk factors
Men aged 70 and older, or younger men with risk factors
The FRAX® tool (Fracture Risk Assessment Tool) complements DXA by estimating 10-year fracture probability based on clinical variables — age, sex, body mass index, prior fractures, parental history of hip fracture, smoking, alcohol use, corticosteroid use, and BMD.
Laboratory investigations (serum calcium, vitamin D, parathyroid hormone, and bone turnover markers) help identify secondary causes of bone loss.
Diagnosing Sarcopenia
Sarcopenia diagnosis is more complex, requiring assessment across three domains:
Muscle strength: Handgrip dynamometry and the five-times chair stand test are the most practical clinical measures.
Muscle mass: DXA provides appendicular lean mass (ALM) — notably, the same machine used for osteoporosis screening can simultaneously provide sarcopenia-relevant data, making it a highly efficient dual-purpose tool.
Physical performance: The gait speed test (normal ≥ 0.8 m/s), Timed Up and Go (TUG) test, 6-minute walk test, and Short Physical Performance Battery (SPPB) quantify functional capacity.
Initial screening can be done with the SARC-F questionnaire, a five-item self-report tool assessing strength, walking assistance, rising from a chair, stair climbing, and falls.
The Impact of Osteoporosis and Sarcopenia on Quality of Life
Both osteoporosis and sarcopenia are major age-related conditions that can dramatically reduce mobility, independence, and long-term healthspan. Although they affect different tissues — bone and muscle — both increase the risk of disability, frailty, falls, hospitalization, and premature mortality.
Osteoporosis: How Weak Bones Affect Daily Life
Osteoporosis is often called the “silent disease” because bone loss develops gradually without symptoms until a fracture occurs. Once fractures happen, the consequences can be life-changing.
Major Consequences of Osteoporosis
Severe pain following hip, spine, or wrist fractures
Loss of height and stooped posture from vertebral compression fractures
Reduced mobility and difficulty performing routine activities
Greater dependence on caregivers and family members
Increased risk of future fractures after the first break
Higher mortality risk, especially after hip fractures in older adults
Loss of confidence and fear of falling
Sarcopenia: The Hidden Driver of Frailty and Weakness
Sarcopenia causes progressive muscle loss, declining strength, and impaired physical performance. Many adults notice symptoms only after mobility and balance have already deteriorated.
Major Consequences of Sarcopenia
Difficulty climbing stairs, rising from chairs, or carrying objects
Reduced walking speed and impaired balance
Increased risk of falls and injury
Development of frailty and physical dependence
Higher hospitalization and institutionalization rates
Loss of independence in daily activities
Lower overall quality of life and physical resilience
The Combined Impact: Osteosarcopenia
When osteoporosis and sarcopenia occur together — a condition known as osteosarcopenia — the health risks multiply significantly. Weak muscles increase the likelihood of falls, while fragile bones increase the risk of fractures after even minor trauma.
Why Osteosarcopenia Is So Dangerous
Greater functional limitations and mobility decline
Markedly higher fall and fracture risk
Accelerated loss of independence
Increased hospitalization and long-term care needs
Higher mortality risk compared with either condition alone
Who Is at Highest Risk?
Osteoporosis Risk Factors
Non-Modifiable Risk Factors
Age over 50 years
Female sex and postmenopausal status
Family history of osteoporosis or fractures
Caucasian and Asian ethnicity
Early menopause or low estrogen exposure
Modifiable Risk Factors
Low calcium and vitamin D intake
Sedentary lifestyle and lack of resistance exercise
Smoking and excessive alcohol use
Long-term corticosteroid therapy
Low body weight or malnutrition
Sarcopenia Risk Factors
Primary Risk Factors
Advanced age, especially after 60
Physical inactivity and prolonged sitting
Inadequate dietary protein intake
Chronic diseases such as Type 2 Diabetes and cardiovascular disease
Chronic inflammation and hormonal decline
Use of glucocorticoids and certain medications
Population Insight
Emerging research suggests that community-dwelling older adults may have significantly higher susceptibility to combined osteoporosis and sarcopenia compared with inpatient and outpatient populations, highlighting the need for earlier screening and preventive intervention.
Treatment: What Actually Works
Managing Osteoporosis
Pharmacological options include:
Bisphosphonates (alendronate, risedronate, zoledronic acid): Reduce bone resorption and lower fracture risk by up to 50%
Denosumab: A monoclonal antibody that suppresses osteoclast activity, particularly effective for postmenopausal osteoporosis
SERMs (selective estrogen receptor modulators, e.g., raloxifene): Mimic estrogen's protective effect on bone
Teriparatide/Abaloparatide: Anabolic agents that stimulate bone formation, used in severe cases
Lifestyle measures form the essential foundation alongside pharmacotherapy:
Weight-bearing exercise (walking, dancing, low-impact aerobics): 30 minutes most days
Calcium intake: 1,000–1,200 mg daily (preferably from food; supplement only if dietary intake is insufficient)
Vitamin D: 800–1,000 IU daily; blood levels should guide dosing
Smoking cessation and limiting alcohol to fewer than two standard drinks per day
Managing Sarcopenia
No pharmacological agent has yet been approved specifically for sarcopenia, though research into myostatin inhibitors, selective androgen receptor modulators (SARMs), and growth hormone secretagogues is ongoing. The current standard of care centers on two pillars:
1. Progressive Resistance Training (PRT): This is the single most evidence-based intervention for sarcopenia. PRT — using free weights, resistance machines, or resistance bands — increases mechanical load on muscle fibers, stimulates muscle protein synthesis, and promotes the release of anabolic hormones including testosterone and IGF-1. Training should target all major muscle groups, 2–3 sessions per week, with progressive increases in load over time. Even adults in their 80s and 90s show meaningful muscle and strength gains with consistent PRT.
2. Nutritional Optimization: The most important nutritional intervention is adequate protein intake: 1.0–1.2 g per kilogram of body weight per day, distributed across all meals rather than concentrated in one. High-quality protein sources — lean meats, poultry, fish, eggs, dairy, legumes, and soy — are preferred. Leucine-rich foods (dairy, whey protein, legumes) are particularly effective at stimulating muscle protein synthesis. Vitamin D supplementation supports both muscle function and calcium absorption, offering dual benefit.
Integrated Management for Osteosarcopenia
For individuals with both conditions, the most efficient approach combines resistance training (for muscle) with weight-bearing activities (for bone), comprehensive nutritional support (protein, calcium, vitamin D), fall-prevention strategies (balance training, home safety modifications, medication review, vision assessment), and regular monitoring of both BMD and muscle function over time.
Cacciatore, Prokopidis, and Schlögl (2025) argue compellingly in European Geriatric Medicine that osteoporosis and sarcopenia must be viewed as "two sides of the same coin" — conditions that share biological drivers and demand integrated, not siloed, clinical responses.
Practical Applications: Your Action Plan Starting Today
You do not need to wait for a diagnosis to take meaningful protective action. These evidence-based steps apply to any adult aged 50 or older:
Week 1–2: Assess Your Risk Complete the SARC-F questionnaire (available from your GP or online). Request a DXA scan if you are over 50, postmenopausal, or have any relevant risk factors. Ask your doctor to calculate your FRAX® score. Have your serum vitamin D and calcium levels checked.
Week 3–4: Build Your Exercise Foundation Begin resistance training twice weekly, even with bodyweight exercises (chair squats, wall push-ups, step-ups). Add daily 30-minute brisk walks. Incorporate balance training: single-leg stands, heel-to-toe walking, or a beginner tai chi class.
Month 2 Onward: Optimize Nutrition Track your daily protein intake using a simple food diary. Aim for at least one high-quality protein source per meal. If blood vitamin D is low, begin supplementation as advised by your doctor. Ensure calcium needs are met through diet first, supplementation second.
Ongoing: Prevent Falls Walk through your home and remove loose rugs, trailing cables, and clutter. Improve lighting in stairways and bathrooms. Install grab rails in the shower and beside the toilet. Have an annual vision check. Review all medications with your pharmacist for those that increase fall risk (sedatives, blood pressure medications, antihistamines).
Frequently Asked Questions
1. Can I have both sarcopenia and osteoporosis at the same time? Yes — and more often than most people realize. Approximately 18% of older adults globally have both conditions simultaneously, a state called osteosarcopenia. This combination significantly increases fall risk, fracture risk, and mortality compared to having either condition alone.
2. What are the earliest warning signs of sarcopenia? Early sarcopenia often appears as subtle functional changes: taking longer to walk the same distance, struggling to open jars, needing the armrests to push yourself out of a chair, or feeling more fatigued than usual after routine activities. These are worth reporting to your doctor — do not dismiss them as "just getting older."
3. Does osteoporosis cause pain? Not typically, until a fracture occurs. That is why it is called the "silent disease." Vertebral compression fractures can cause sudden, severe back pain, but many occur without any noticeable symptoms at all. This makes regular DXA screening essential for at-risk adults.
4. What is the best exercise for both conditions at once? A combination of progressive resistance training (for muscle and bone-stimulating mechanical load) and weight-bearing aerobic exercise (walking, stair climbing, low-impact aerobics) provides the most comprehensive benefit. Balance training — tai chi, yoga, single-leg standing — adds the critical layer of fall prevention.
5. How much protein do I actually need after age 60? Most evidence supports 1.0–1.2 grams of protein per kilogram of body weight per day for older adults — substantially more than the general adult recommendation. For a 70 kg (154 lb) adult, that means 70–84 grams of protein daily. Distribute intake across meals rather than consuming it all at dinner, as muscles can only utilize a limited amount at any one time.
6. Are there medications specifically for sarcopenia? Not yet, though several are in clinical trials. Current treatment focuses on progressive resistance exercise and adequate protein and vitamin D intake. Some physicians may prescribe testosterone or other hormonal therapies in specific cases, but these are not routinely recommended for sarcopenia alone.
7. At what age should I start thinking about these conditions? Prevention should ideally begin in your 30s and 40s — when bone density peaks and muscle mass is at its highest. However, it is never too late to start. Meaningful improvements in bone density and muscle strength are achievable even in adults in their 70s, 80s, and beyond with consistent exercise and nutrition.
Clinical pearls
1. Osteosarcopenia Synergy
Clinical Pearl: Sarcopenia and osteoporosis must no longer be managed as distinct, siloed conditions. The coexistence of both—now formally classified as osteosarcopenia—exerts a dangerous synergistic effect. Recent cohort data (Liu et al., 2025) demonstrates that having both conditions produces an additive effect on all-cause mortality that increases risk by up to 75%, vastly exceeding the independent risk of either disease alone.
Think of your muscles and bones as a team. If one gets weak, the other struggles; if both break down at the same time, the danger multiplies. Having muscle loss and bone thinning together doesn't just double your risks—it skyrockets your overall health risk by 75%. Treating them together is a medical necessity, not an option.
2. The DXA Scan is a Dual-Purpose Efficiency Tool
Clinical Pearl: Maximize diagnostic efficiency by utilizing the Dual-Energy X-ray Absorptiometry (DXA) scan for more than just bone mineral density (BMD). The exact same machine can simultaneously measure Appendicular Lean Mass (ALM) to evaluate for muscle wasting. When ordering a DXA for an at-risk patient over 50, ensure body composition software is utilized to capture both baseline metrics in a single clinical encounter.
There is no need for a dozen complicated tests. The very same quick, painless bone density scan (DXA) used to check your bones can also measure your muscle mass. It is a highly efficient "two-for-one" test that tells us exactly what is happening under the surface.
3. The "Paradoxical" High Risk in Males
Clinical Pearl: Do not let gender bias cloud screening choices. While osteoporosis is epidemiologically more prevalent in postmenopausal women, the relative risk correlation when sarcopenia is present is paradoxically higher in men. Present data shows that males with sarcopenia carry a 4.74 times higher risk of comorbid osteoporosis, compared to 3.46 times in females (Jin et al., 2025). Sarcopenic men require immediate bone density screening.
While we often think of bone thinning as a woman's health issue, men with muscle loss are actually at a remarkably high risk for weak bones. If you are a man noticing a loss in physical strength or grip, your bones may be thinning even faster than a woman's would under the same conditions.
4. Mechanical Loading Dependency (Bones Need Muscle Force)
Clinical Pearl: Bone mineral density cannot be fully optimized in a muscular vacuum. Bone remodeling relies heavily on mechanotransduction—the physical pull of muscle contracting against bone tissue. Sarcopenia directly removes this primary physiological stimulus for osteoblast (bone-building cell) activity. Therefore, treating osteoporosis with pharmacotherapy alone while ignoring muscle wasting is clinically sub-optimal.
Medications and calcium are great, but bones actually require the physical "tug" of strong muscles to stay dense and healthy. When you lose muscle, your bones lose their natural signal to rebuild. You cannot fully fix your bones without also rebuilding your muscles.
5. Overcoming Anabolic Resistance with 1.2g/kg Protein Target
Clinical Pearl: Aging skeletal muscle exhibits "anabolic resistance," meaning older adults require a higher concentration of systemic amino acids to stimulate muscle protein synthesis compared to younger populations. To counter this, adults over 50 require 1.0 to 1.2 g/kg/day of high-quality protein, evenly distributed across meals (aiming for roughly 25–30g of protein per meal to cross the "leucine trigger" threshold required to spark muscle synthesis).
As we age, our bodies become less efficient at turning dietary protein into muscle. To fight this, adults over 50 actually need more protein than younger adults—about 1 to 1.2 grams for every kilogram of body weight. Instead of saving all your protein for dinner, space it out through the day so your muscles get a steady supply to rebuild.
6. Functional Capacity Trumps Mass Alone (The SARC-F Shift)
Clinical Pearl: Sarcopenia diagnosis is fundamentally a metric of function, not just muscle volume. A patient can have normal-looking muscle bulk but severely impaired muscle quality and power. Clinicians should prioritize simple, rapid functional biomarkers in office visits: handgrip dynamometry, gait speed (< 0.8 m/s), and the 5-times chair stand test. Initial stratification can be efficiently managed via the 5-item SARC-F self-report questionnaire.
Preventing disability isn't about looking like a bodybuilder; it's about how your muscles perform. Subtle clues like struggling to open jars, moving a bit slower, or needing to push off the armrests to get out of a chair are early warning signs that your muscle quality is slipping. Pay attention to your real-world strength, not just your weight.
Clinician’s Perspective:
In everyday clinical practice, Sarcopenia and osteoporosis rarely announce themselves dramatically in their early stages. Instead, they appear subtly — a slower gait, difficulty rising from a chair, reduced grip strength, mild weight loss, increasing fatigue, or a growing fear of falling. Unfortunately, many patients — and sometimes clinicians — normalize these warning signs as “just aging.”
Consider a common real-world scenario: a 72-year-old man with type 2 diabetes, abdominal obesity, low physical activity, and progressive weakness presents after a minor fall while stepping off a curb. Imaging reveals a vertebral compression fracture. Further evaluation shows osteopenia bordering on osteoporosis, markedly reduced grip strength, slow gait speed, and low appendicular lean mass on DXA. In retrospect, the fracture was not the beginning of the disease — it was the late manifestation of years of silent musculoskeletal decline.
Clinically, this changes how we should approach aging adults. Sarcopenia and osteoporosis are not isolated orthopedic conditions; they are systemic markers of declining biological resilience. Patients with low muscle strength are more likely to fall. Patients with fragile bones are more likely to fracture. Immobilization after fracture accelerates further muscle wasting, insulin resistance, inflammation, and frailty — creating a self-perpetuating cycle.
This is why early screening matters. Simple tools such as gait-speed testing, chair-stand assessment, SARC-F questionnaires, DXA scanning, vitamin D measurement, and FRAX® scoring can identify high-risk patients years before catastrophic disability occurs.
Perhaps most importantly, these conditions remain modifiable. Resistance training, adequate protein intake, metabolic optimization, balance training, and fall-prevention strategies are not merely lifestyle advice — they are frontline preventive medicine for preserving independence, mobility, and healthspan in aging adults.
This information is for educational purposes only and should not replace professional medical advice. Always consult with your healthcare provider for personalized recommendations based on your individual health status and risk factors.
Related Articles
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | DR T S DIDWAL
References
Cacciatore, S., Prokopidis, K., & Schlögl, M. (2025). Osteoporosis and sarcopenia: two sides of the same coin. European Geriatric Medicine, 16, 1749–1752. https://doi.org/10.1007/s41999-025-01275-z
Chen, S., Xu, X., Gong, H., Chen, R., Guan, L., Yan, X., Zhou, L., Yang, Y., Wang, J., Zhou, J., Zou, C., & Huang, P. (2024). Global epidemiological features and impact of osteosarcopenia: A comprehensive meta-analysis and systematic review. Journal of Cachexia, Sarcopenia and Muscle, 15(1), 8–20. https://doi.org/10.1002/jcsm.13392
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., Cooper, C., Landi, F., Rolland, Y., Sayer, A. A., Schneider, S. M., Sieber, C. C., Topinkova, E., Vandewoude, M., Visser, M., Zamboni, M., & Writing Group for EWGSOP2. (2019). Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
Jin, S., Zheng, F., Liu, H., Liu, L., & Yu, J. (2025). The correlation between sarcopenia and osteoporosis in the elderly: A systematic review and meta-analysis. Frontiers in Medicine, 12, 1603879. https://doi.org/10.3389/fmed.2025.1603879
Liu, Y., Chen, H., Zhang, P., et al. (2025). The additive effect of sarcopenia and osteoporosis on all-cause mortality: A cohort analysis in a U.S. population. Scientific Reports, 15, 43408. https://doi.org/10.1038/s41598-025-00003-8
Zhan, Z., Zhang, Y., Wu, J., et al. (2025). Predictive efficacy of different diagnostic criteria for sarcopenia in osteoporosis and fractures. Scientific Reports, 15, 9473. https://doi.org/10.1038/s41598-025-93988-1