How Muscle Strength Correlates with Mortality Risk: Evidence from 7 Major Studies
Does strength training reduce mortality? Discover what 7 major studies reveal about muscle strength, longevity, and how to lower your risk of death.
EXERCISEAGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/5/202615 min read
What is the link between muscle strength and longevity?
Muscle strength is strongly associated with a lower risk of death, cardiovascular disease, and disability.
Randomized controlled trials consistently show that resistance training improves muscle strength, insulin sensitivity, and functional capacity, supporting a causal pathway between strength gains and improved health outcomes.
Muscle strength is not just a marker of fitness—it is a clinically meaningful predictor of survival, functional independence, and chronic disease risk. Routine assessment (e.g., grip strength) and early intervention with resistance training should be considered part of preventive healthcare, especially after midlife.
Key Facts About Muscle Strength and Longevity
Low muscle strength is linked to higher all-cause mortality
Grip strength is a validated clinical biomarker of aging
30–60 minutes/week of resistance training reduces disease risk
Muscle strength influences:
Insulin sensitivity
Inflammation
Cardiovascular health
Muscle power declines faster than strength with age
Sarcopenia affects 10–27% of adults over 60
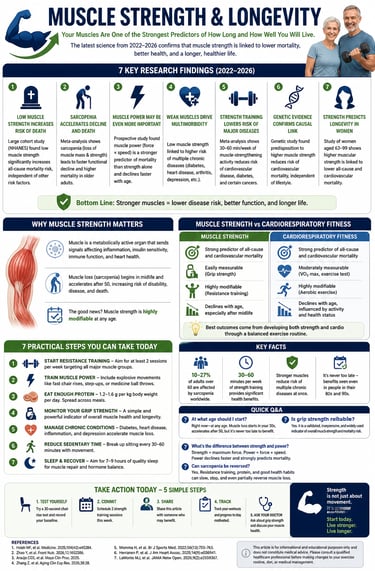
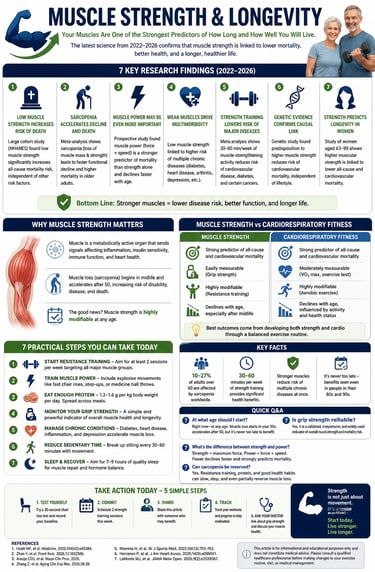
Muscle Strength vs Cardiorespiratory Fitness
Muscle Strength
Strong predictor of all-cause and cardiovascular mortality
Easily measurable using tools like grip strength dynamometry
Highly modifiable through resistance training
Declines progressively with age, especially after midlife
Cardiorespiratory Fitness
Strong predictor of mortality and cardiovascular health
Measurement requires exercise testing (e.g., VO₂ max), making it moderately accessible
Highly modifiable through aerobic exercise
Also declines with age, influenced by physical activity levels and health status
Both muscle strength and cardiorespiratory fitness are independent and complementary predictors of longevity. Optimal health outcomes are achieved when both are developed together through combined resistance and aerobic training.
Muscle strength is one of the strongest predictors of how long and how well you will live.
Recent evidence from seven major studies (2022–2026) shows that higher muscle strength is consistently linked to significantly lower risk of all-cause mortality, cardiovascular death, and multiple chronic diseases. Low muscle strength and sarcopenia, on the other hand, are associated with higher mortality, faster functional decline, and increased multimorbidity. When most people think about healthy aging, they think about heart health, blood pressure, or blood sugar. Rarely do they think about the size and strength of their muscles. But the science tells a different story.
Muscle tissue is now understood to be a metabolically active endocrine organ — meaning it sends hormonal signals throughout the body that regulate inflammation, insulin sensitivity, immune function, and cardiovascular health. When muscle is lost or weakened, these signals deteriorate, setting off a cascade of health problems that accelerate biological aging and increase the risk of premature death.
The condition of age-related muscle loss is called sarcopenia, and it is far more common — and far more dangerous — than most people realize.
Key findings include:
Grip strength serves as a reliable, easy-to-measure biomarker of biological aging and longevity.
Muscle power (the ability to generate force quickly) may be an even stronger predictor of mortality than muscle strength alone.
Just 30–60 minutes per week of resistance training provides meaningful protection against major diseases and premature death.
Benefits apply to both men and women and remain significant even in people in their 80s and 90s.
Genetic studies suggest the relationship between muscle strength and lower cardiovascular mortality is likely causal, not just correlational.
Bottom Line: Maintaining or building muscle strength through resistance training is one of the most effective, modifiable strategies available for extending both lifespan and healthspan. It is never too early or too late to start.
What the Research Tells Us: Seven Key Studies
1. Low Muscle Strength Is a Direct Risk Factor for Early Death
A large-scale retrospective cohort study using data from the National Health and Nutrition Examination Survey (NHANES) found that individuals with low muscle strength faced significantly higher mortality risk compared to those with adequate strength (Hsieh et al., 2025). The study, published in Medicine, analyzed a nationally representative population and demonstrated that muscle strength — measured through grip strength and functional performance — independently predicted all-cause mortality even after adjusting for age, sex, body mass index, and chronic disease status.
In plain language: weak muscles kill, and the relationship holds regardless of whether someone appears otherwise healthy.
2. Sarcopenia Accelerates Functional Decline and Death in Older Adults
A sweeping systematic review and meta-analysis published in Frontiers in Nutrition (Zhao et al., 2026) pooled data from multiple long-term studies of community-dwelling older adults. The findings were sobering: sarcopenia — the loss of both muscle mass and muscle strength — was strongly associated with accelerated functional decline (the progressive loss of ability to perform daily activities) and significantly increased mortality risk.
What makes this finding particularly alarming is that sarcopenia often begins silently in midlife, accelerating after the age of 50 and becoming clinically significant in the 60s and 70s. By the time most people notice the effects, substantial damage may already have occurred. Early detection and intervention are therefore critical.
3. Muscle Power May Be Even More Important Than Muscle Strength
Most people understand strength — how much you can lift. But a groundbreaking prospective cohort study published in Mayo Clinic Proceedings (Araújo et al., 2025) made a finer and important distinction: muscle power — the ability to exert force rapidly, such as rising quickly from a chair or climbing stairs with speed — may be an even more sensitive predictor of mortality than raw muscle strength alone.
The study followed middle-aged and older men and women and found that those with lower muscle power faced elevated mortality risk, and that power declined faster with age than strength did. This has significant clinical implications: rehabilitation programs and exercise regimens that focus only on how much weight someone can lift may be missing a critical piece of the puzzle.
4. Weak Muscles Drive Multimorbidity — Having Multiple Diseases at Once
One of the most significant emerging findings comes from a prospective cohort study of middle-aged and older adults in China (Zhang et al., 2026), published in Aging Clinical and Experimental Research. The study found that low muscle strength was strongly associated with multimorbidity — the simultaneous presence of two or more chronic diseases such as diabetes, heart disease, arthritis, or depression.
This is a critical finding because multimorbidity is the leading driver of disability, poor quality of life, and healthcare costs worldwide. Rather than treating each disease separately, this research suggests that targeting muscle strength could simultaneously reduce the risk of multiple conditions — essentially hitting many birds with one stone.
5. Muscle-Strengthening Activity Lowers Risk of Major Non-Communicable Diseases
A landmark systematic review and meta-analysis published in the British Journal of Sports Medicine (Momma et al., 2022) analyzed data from cohort studies and found that regular muscle-strengthening activities — such as resistance training, bodyweight exercises, or even heavy gardening — were associated with meaningfully lower risk of developing or dying from major non-communicable diseases (NCDs), including cardiovascular disease, type 2 diabetes, and certain cancers.
The dose-response relationship was particularly noteworthy: even modest amounts of muscle-strengthening activity — as little as 30–60 minutes per week — provided substantial protective benefits. You do not need to be in a gym seven days a week to begin reaping rewards.
6. Genetic Evidence Confirms the Causal Link Between Muscle Strength and Heart Health
Skeptics of observational research often argue that people with stronger muscles may simply be healthier to begin with — a classic chicken-and-egg problem. A rigorous longitudinal cohort study from Finland (Herranen et al., 2025), published in the Journal of the American Heart Association, addressed this head-on using Mendelian randomization — a method that uses genetic data to establish causal relationships rather than mere associations.
The study found that a genetic predisposition to higher muscle strength was associated with a lower risk of cardiovascular disease mortality in men, independent of leisure-time physical activity in adulthood. In other words, even accounting for lifestyle, the biological capacity for strength itself appears to be cardioprotective. This provides some of the strongest evidence to date that the relationship between muscle strength and mortality is genuinely causal, not merely correlational.
7. Muscle Strength Predicts Longevity in Women Aged 63–99
Women are often underrepresented in muscle strength research, which has historically focused more heavily on male populations. A major study published in JAMA Network Open (LaMonte et al., 2026) specifically examined muscular strength and mortality in women aged 63 to 99 years — a broad and clinically important age range.
The results confirmed that higher muscular strength was associated with significantly lower all-cause and cardiovascular mortality in older women. Critically, the protective effect was seen across all age groups within the study, including women in their 80s and 90s, suggesting it is never too late to benefit from building or maintaining muscle strength.
Clinical Takeaways: Muscle Strength and Longevity
1. Muscle strength is an independent predictor of mortality
Large cohort data (e.g., NHANES) show that low muscle strength predicts all-cause mortality independent of age, BMI, and comorbidities.
➡️ Clinical implication: Muscle strength should be considered alongside traditional vital risk markers in routine assessment.
2. Sarcopenia is a high-impact, underdiagnosed condition
Meta-analytic evidence confirms that sarcopenia is strongly associated with functional decline, frailty, and premature death.
➡️ Clinical implication: Early screening (e.g., grip strength, gait speed) should be integrated into midlife and geriatric care.
3. Muscle power is a critical—and often overlooked—risk marker
Prospective data suggest muscle power (force × speed) may predict mortality more sensitively than strength alone, and declines earlier with age.
➡️ Clinical implication: Functional tests (chair rise, stair climb) and power-based training should complement traditional strength programs.
4. Low muscle strength contributes to multimorbidity
Cohort studies demonstrate a strong association between weak muscle strength and increased risk of multiple coexisting chronic diseases.
➡️ Clinical implication: Improving muscle strength may act as a shared upstream intervention across cardiometabolic and musculoskeletal diseases.
5. Even modest resistance training yields substantial health benefits
Meta-analysis evidence shows that 30–60 minutes/week of muscle-strengthening activity significantly reduces the risk of cardiovascular disease, diabetes, and cancer mortality.
➡️ Clinical implication: Low-dose, scalable interventions can be prescribed broadly—even in resource-limited settings.
6. Genetic evidence supports a likely causal relationship
Mendelian randomization data indicate that a genetic predisposition to higher muscle strength is associated with lower cardiovascular mortality, independent of lifestyle factors.
➡️ Clinical implication: Strength is not just a marker of health—it is likely a biologically relevant determinant, strengthening the rationale for intervention.
7. Benefits extend across age and sex—including very old adults
Evidence in women aged 63–99 shows that higher muscle strength is associated with lower mortality even in advanced age.
➡️ Clinical implication: It is never too late to intervene—strength training should be encouraged across the entire lifespan, including the oldest populations.
Clinical Bottom Line
Muscle strength is emerging as a central, modifiable pillar of preventive medicine, influencing mortality, multimorbidity, and functional independence. Routine assessment and targeted intervention should be considered standard components of modern clinical practice, aligned with recommendations from organizations such as the World Health Organization and American College of Sports Medicine.
Practical Applications: What You Can Do Starting Today
✅ 1. Start Resistance Training — At Any Age
The evidence is unambiguous: resistance training is the most effective intervention for building and maintaining muscle strength. Aim for at least 2 sessions per week, targeting all major muscle groups (legs, core, back, arms, and chest). Beginners can start with bodyweight exercises such as squats, lunges, push-ups, and wall sits before progressing to weights or resistance bands.
✅ 2. Don't Neglect Muscle Power
Given the findings of Araújo et al. (2025), your exercise routine should also include explosive movements that train muscle power — the ability to move forcefully and quickly. Simple examples include:
Chair rises performed as fast as safely possible
Step-ups with an emphasis on speed
Light medicine ball throws
Walking up stairs briskly
✅ 3. Eat Enough Protein
Muscle cannot be built or maintained without adequate dietary protein. Research supports a target of 1.2–1.6 grams of protein per kilogram of body weight per day for older adults engaged in resistance training. Distribute protein intake across meals rather than consuming it all at once. Good sources include eggs, dairy, legumes, fish, poultry, and lean red meat.
✅ 4. Monitor Your Grip Strength
Grip strength — easily measured with an inexpensive hand dynamometer — is one of the most reliable proxies for overall muscle strength and has been validated as a predictor of mortality in multiple studies. Ask your doctor about including grip strength measurement in your next check-up, or purchase a home dynamometer to track trends over time.
✅ 5. Address the Diseases That Accelerate Muscle Loss
Conditions such as type 2 diabetes, chronic inflammation, heart failure, and depression all accelerate sarcopenia. Working with your healthcare team to manage these conditions proactively will help protect your muscle health. Conversely, since Zhang et al. (2026) showed that stronger muscles reduce multimorbidity risk, improving muscle strength is itself a strategy for disease prevention.
✅ 6. Reduce Sedentary Time
Prolonged sitting accelerates muscle atrophy. Break up seated periods every 30–60 minutes with brief activity — even a short walk or set of standing calf raises can help. Wearable fitness trackers can be a helpful accountability tool.
✅ 7. Sleep and Recover Adequately
Muscle repair and growth happen primarily during sleep. Chronic sleep deprivation suppresses anabolic hormones (particularly growth hormone and testosterone) that are essential for maintaining muscle mass. Aim for 7–9 hours of quality sleep per night.
Frequently Asked Questions (FAQs)
FAQ 1: At what age should I start worrying about muscle strength and longevity?
The honest answer is: right now, regardless of your age. Muscle loss typically begins around age 30–35 and accelerates after 50. However, as LaMonte et al. (2026) demonstrated, protective benefits from maintaining or building strength are seen even in individuals in their 80s and 90s. Starting early is ideal, but starting late is infinitely better than not starting at all.
FAQ 2: Is grip strength really a reliable way to measure my overall muscle health?
Yes — grip strength has been validated in dozens of large-scale studies as a powerful proxy for overall skeletal muscle strength. The NHANES study by Hsieh et al. (2025) is among the many that used it as a key measure. It is inexpensive, quick, and highly reproducible, which is why clinicians increasingly recommend it as a routine vital sign in older adults.
FAQ 3: What is the difference between muscle strength and muscle power, and why does it matter?
Muscle strength is the maximum force your muscles can produce — for example, the heaviest weight you can lift once. Muscle power is force multiplied by speed — how quickly you can produce that force, like getting up from a chair rapidly or catching yourself from a fall. Araújo et al. (2025) found that power may be an even more sensitive mortality predictor than strength, and power declines faster with age. Training programs should address both.
FAQ 4: Can women benefit as much as men from strength training for longevity?
Absolutely. The study by LaMonte et al. (2026) specifically demonstrated that higher muscular strength predicts lower mortality in women aged 63–99. Meanwhile, the genetic study by Herranen et al. (2025) focused on men, but the broader literature supports similar benefits across sexes. Women may actually have more to gain from strength training relative to baseline, since they tend to have lower muscle mass and are at higher risk of sarcopenia-related disability.
FAQ 5: How much resistance training is needed to get meaningful mortality benefits?
The meta-analysis by Momma et al. (2022) found significant benefits from as little as 30–60 minutes of muscle-strengthening activity per week — far less than most people assume. Consistency over years matters more than the intensity of any individual session. Even simple bodyweight exercises done regularly provide measurable protection.
FAQ 6: Can sarcopenia be reversed once it has started?
Yes — to a meaningful degree. While some age-related muscle loss is inevitable, research consistently shows that progressive resistance training, adequate protein intake, and management of underlying health conditions can significantly slow progression, partially restore lost muscle mass, and — critically — improve muscle strength and function even in advanced sarcopenia. You are never too old or too weak to begin.
FAQ 7: Should I consult my doctor before starting a strength training program?
If you have existing cardiovascular disease, joint problems, or other significant health conditions, a brief check-in with your doctor or a physiotherapist before starting is wise. However, for most people, starting with low-intensity bodyweight exercises is safe without prior medical clearance. The risk of not exercising vastly outweighs the risk of beginning a sensible, graduated training program.
Clinical pearls
1. The "Metabolic Sink" Effect
Scientific Perspective: Skeletal muscle is the primary site for postprandial glucose disposal (roughly 80%). Loss of muscle mass (sarcopenia) reduces the body's "metabolic sink," directly increasing the risk of insulin resistance and Type 2 Diabetes, regardless of adiposity.
Think of your muscles as a sponge for blood sugar. The more muscle you have, the more "fuel" your body can burn even while you’re sitting down. When you lose muscle, your body loses its best tool for keeping your blood sugar in check.
2. Strength vs. Power: The Velocity Factor
Scientific Perspective: While absolute force production (strength) is critical, the rate of force development (power) declines at nearly double the rate of strength as we age. Type II (fast-twitch) fibers atrophy preferentially, making power a more sensitive predictor of fall risk and functional independence.
It’s not just about how much you can lift; it’s about how fast you can move. Being able to catch yourself during a trip or get out of a low car requires "power." To keep your independence, you need to practice moving with a bit of "zip" or speed, not just lifting heavy things slowly.
3. The Grip Strength "Vital Sign"
Scientific Perspective: Handgrip strength serves as a highly reliable proxy for global muscular force and central nervous system integrity. It correlates strongly with biological age and is a better predictor of cardiovascular mortality than systolic blood pressure in several large cohorts.
Your handgrip is like a "check engine light" for your whole body. If your grip is getting weaker, it’s a sign that your heart and nervous system might be struggling too. It’s one of the easiest health tests you can do to see how well you are aging.
4. The Anabolic Resistance of Aging
Scientific Perspective: Older adults experience "anabolic resistance," where the muscle becomes less responsive to protein intake and exercise. To overcome this, protein boluses must be larger (roughly 0.4g/kg per meal) and contain higher concentrations of the amino acid Leucine to trigger muscle protein synthesis.
As we get older, our muscles become "hard of hearing." To get them to grow, you have to "yell" louder by eating more protein at each meal—especially after a workout. A small yogurt isn't enough anymore; you need a solid serving of protein to tell your muscles to stay strong.
5. Myokines: Exercise as Medicine
Scientific Perspective: Contracting muscles secrete myokines (like IL-6 and Irisin) that exert anti-inflammatory effects and cross the blood-brain barrier to stimulate BDNF (Brain-Derived Neurotrophic Factor). This makes resistance training a systemic "polypill" for both heart and brain health.
Every time you lift weights, your muscles release "pharmacy chemicals" into your bloodstream. These natural chemicals travel to your brain to improve your mood and memory, and to your heart to reduce inflammation. Muscle is your body’s built-in medicine cabinet.
The Bottom Line: Strength Is Survival
The science is in, and it is consistent across populations, countries, sexes, age groups, and research methodologies: your muscle strength is among the most powerful determinants of how long you will live and how well you will age.
Low muscle strength increases your risk of dying from cardiovascular disease, accelerates functional decline, drives the development of multiple chronic diseases simultaneously, and predicts poor outcomes even in those who appear otherwise healthy. Conversely, maintaining or building muscle strength — through regular resistance training, adequate nutrition, and healthy lifestyle habits — provides robust, dose-responsive protection against all of these outcomes.
And perhaps most encouragingly: you can start today. Whether you are 35 or 85, your muscles are responsive to training. The investment of even a few hours per week in strength-building activity could be among the most important health decisions you ever make.
The best time to start building strength was 20 years ago. The second-best time is right now."
Author’s Note
This article was developed to bridge the gap between emerging scientific evidence and real-world clinical application in the field of muscle health and longevity. The content is based on a critical synthesis of recent peer-reviewed studies (2022–2026), including large cohort analyses, systematic reviews, and genetic investigations exploring the relationship between muscle strength, chronic disease risk, and mortality.
While the evidence consistently demonstrates strong associations between low muscle strength and adverse health outcomes, it is important to recognize that much of the current literature remains observational in nature. Although advanced methodologies such as Mendelian randomization strengthen causal inference, findings should still be interpreted within the broader context of clinical judgment and individual variability.
From a clinical perspective, muscle strength represents a highly modifiable and often underappreciated determinant of health. Unlike many traditional risk factors, it can be improved at nearly any age through targeted interventions such as resistance training, adequate protein intake, and reduction of sedentary behavior. As such, integrating muscle health into routine preventive care may offer substantial benefits for both longevity and quality of life.
This article is intended for educational purposes only and should not replace personalized medical advice. Readers are encouraged to consult qualified healthcare professionals before making significant changes to their exercise, nutrition, or medical management strategies.
This article is intended for informational and educational purposes only. It does not constitute medical advice. Please consult a qualified healthcare professional before making changes to your exercise routine, diet, or medical management.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
.Related Articles
Why Strength Training Reduces Inflammation and May Prevent Most Chronic Diseases
The Aging Muscle Paradox: How Senescent Cells Cause Insulin Resistance and The Strategies to Reverse It | DR T S DIDWAL
VO2 Max & Longevity: The Ultimate Guide to Living Longer | DR T S DIDWAL
References
Araújo, C. G. S., de Castro, C. L. B., & et al. (2025). Muscle power versus strength as a predictor of mortality in middle-aged and older men and women: A prospective cohort study. Mayo Clinic Proceedings. Advance online publication. https://doi.org/10.1016/j.mayocp.2025.02.004
Herranen, P., et al. (2025). Genetic liability to higher muscle strength associates with a lower risk of cardiovascular disease mortality in men irrespective of leisure-time physical activity in adulthood: A longitudinal cohort study. Journal of the American Heart Association, 14(9), e036941. https://doi.org/10.1161/JAHA.124.036941
Hsieh, M. F., Wang, S. I., Hsieh, H. F., Huang, M. Z., & Wang, H. H. (2025). Low muscle strength and mortality: Key risk factors in the National Health and Nutrition Examination Survey retrospective cohort study. Medicine, 104(42), e45284. https://doi.org/10.1097/MD.0000000000045284
LaMonte, M. J., Hyde, E. T., Nguyen, S., et al. (2026). Muscular strength and mortality in women aged 63 to 99 years. JAMA Network Open, 9(2), e2559367. https://doi.org/10.1001/jamanetworkopen.2025.59367
Momma, H., et al. (2022). Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: A systematic review and meta-analysis of cohort studies. British Journal of Sports Medicine, 56(13), 755–763. https://doi.org/10.1136/bjsports-2021-105061
Zhang, Z., Zhu, L., & Chen, Z. (2026). Muscle strength and the risk of multimorbidity in middle-aged and older Chinese adults: A prospective cohort study. Aging Clinical and Experimental Research, 38, 28. https://doi.org/10.1007/s40520-025-03276-1
Zhao, Y., Jiang, Y., Guo, Y., Pan, W., Tian, W., Tang, L., & Feng, X. (2026). Long-term impact of sarcopenia on functional decline and mortality in community-dwelling older adults: A systematic review and meta-analysis. Frontiers in Nutrition, 12, 1652386. https://doi.org/10.3389/fnut.2025.1652386