Best Exercises for Osteoporosis: How to Build Bone Density and Prevent Fractures Naturally
Discover the best exercises for osteoporosis backed by 2026 research. Learn how resistance training, balance work, and HiRIT build bone density safely.
EXERCISESARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/25/202622 min read
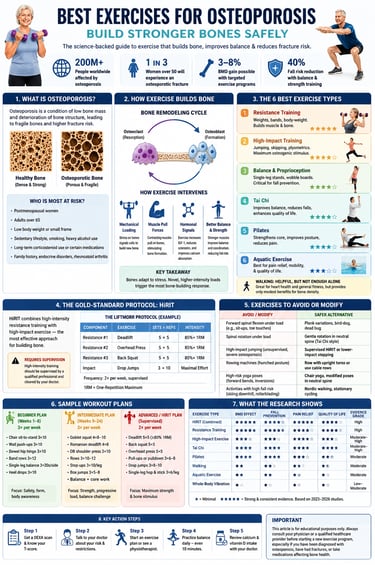
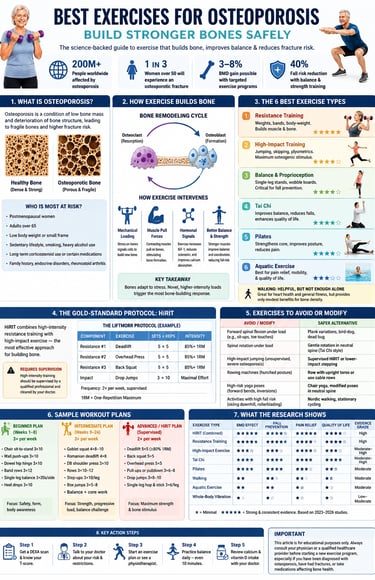
The best exercises for osteoporosis are resistance training, weight-bearing impact exercise, balance training, and combined high-intensity resistance and impact training (HiRIT). Research shows these exercises can improve bone mineral density, strengthen muscles, reduce falls, and lower fracture risk when performed safely and consistently.
Clinical Pearls
1. Resistance training is the foundation for building stronger bones.
Progressive weight training or resistance exercises (squats, deadlifts, overhead presses) apply mechanical loading that directly stimulates osteoblasts to form new bone. Studies consistently show meaningful gains in lumbar spine and hip bone mineral density when performed 2–3 times per week at moderate to high intensity.
2. Combine resistance training with impact exercise for the best results.
The HiRIT approach (high-intensity resistance + impact training) produces superior bone density improvements compared to either modality alone. When supervised and properly progressed, this combination safely strengthens bone, improves muscle power, and enhances physical function in postmenopausal women.
3. Balance and fall prevention training is just as important as building bone density.
Single-leg stands, Tai Chi, and proprioceptive exercises can reduce fall risk by up to 40%. Since most osteoporotic fractures occur after a fall, improving balance and coordination provides critical real-world protection, even if bone density gains are modest.
4. Avoid spinal flexion under load — protect your spine.
Exercises like traditional sit-ups, crunches, or toe touches increase fracture risk in the thoracic and lumbar spine. Safer alternatives include planks, bird-dog, and dead bug exercises that strengthen the core while maintaining a neutral spine.
5. Walking is beneficial but not enough on its own.
While brisk walking supports general health and offers modest lumbar spine benefits, it does not provide sufficient novel mechanical loading to optimally stimulate bone formation. For osteoporosis management, combine walking with resistance training and targeted impact or balance work.
6. Start safely and progress gradually under guidance.
Exercise is safe and highly effective for both osteopenia and osteoporosis when tailored appropriately. Begin with a beginner program or professional supervision (especially for HiRIT), get medical clearance, and focus on consistent long-term practice — measurable bone and functional improvements typically appear within 3–24 months.
Why Exercise May Be the Most Powerful “Medicine” for Your Bones
A single fall can change a life forever. For millions of older adults, osteoporosis turns ordinary movements — bending to tie a shoe, stepping off a curb, lifting groceries — into potential fracture risks. Hip fractures are especially devastating: nearly 1 in 4 older adults die within a year after a hip fracture, while many others lose long-term independence and mobility (National Osteoporosis Foundation, 2023; WHO, 2022). Yet despite how serious osteoporosis can become, many people never realize their bones are weakening until the first fracture occurs.
The encouraging news is that bone is not dead tissue. It is living, metabolically active tissue that constantly rebuilds itself in response to stress, movement, and muscle contraction. Research over the last decade — particularly newer studies published between 2023 and 2026 — shows that the right types of exercise can slow bone loss, improve bone mineral density (BMD), strengthen muscles, enhance balance, and dramatically reduce fall risk (Lu et al., 2026; Zheng et al., 2025). In some individuals, targeted exercise programs may even partially reverse osteopenia and produce measurable gains in bone density.
But here is the critical detail most people are never told: not all exercise protects bones equally. Some forms of exercise provide little osteogenic stimulus, while others can significantly strengthen the spine and hips — the two most common fracture sites. Certain movements may even increase fracture risk if performed incorrectly in people with fragile bones (Bae et al., 2023).
Understanding the difference can determine whether exercise merely burns calories — or truly helps rebuild stronger, safer bones.
But here is the critical detail most people are never told: not all exercise protects bones equally. Some forms of exercise provide little osteogenic stimulus, while others can significantly strengthen the spine and hips — the two most common fracture sites. Certain movements may even increase fracture risk if performed incorrectly in people with fragile bones (Bae et al., 2023).
Understanding the difference can determine whether exercise merely burns calories — or truly helps rebuild stronger, safer bones.
200M+ People worldwide affected by osteoporosis
1 in 3 Women over 50 will experience an osteoporotic fracture
3–8% BMD gain possible with targeted exercise programs
40% Fall risk reduction with balance & strength training
1. What Is Osteoporosis? Key Facts You Need to Know
Osteoporosis is a skeletal condition characterized by reduced bone mineral density (BMD) and deterioration of bone microstructure, making bones fragile and prone to fracture. Healthy bone resembles a dense honeycomb; in osteoporosis, the spaces in that honeycomb widen, creating a more porous, weakened structure.
The condition is often called a "silent disease" because it develops without symptoms until a fracture occurs — most commonly in the hip, wrist, or spine. A hip fracture, in particular, can have devastating consequences: up to 25% of older adults who suffer one do not survive the following year.
⚠ Osteopenia vs. Osteoporosis
Osteopenia is lower-than-normal bone density that hasn't yet crossed the clinical threshold for osteoporosis. Both conditions respond well to the same types of exercise intervention, though osteopenia offers a bigger preventive window. A 2026 network meta-analysis by Lu et al. confirmed that exercise benefits BMD, balance, pain, and quality of life in both groups.
Who Is Most at Risk?
Postmenopausal women — the decline in estrogen after menopause sharply accelerates bone loss. Women typically reach peak bone mass in their early 20s, then experience a gradual decline.
Adults over 65 of any gender
People with low body weight or a small skeletal frame
Those with sedentary lifestyles, smokers, and heavy alcohol users
People on long-term corticosteroids (prednisone, etc.) or certain other medications
Those with a family history, endocrine disorders (hyperthyroidism, diabetes), or rheumatoid arthritis
2. How Exercise Actually Builds Bone: The Science
Bone is living tissue that constantly remodels itself through a carefully balanced process of bone resorption (breakdown, by osteoclasts) and bone formation (building, by osteoblasts). Osteoporosis tips this balance toward resorption — more bone is broken down than built.
Exercise counteracts this in several interconnected ways:
Mechanical Loading: The Core Mechanism
When your bones experience mechanical stress — from impact, body weight, or the pull of contracting muscles — they flex microscopically. Osteocytes (bone cells embedded in the bone matrix) sense this deformation and signal osteoblasts to lay down new bone tissue. This is called the mechanostat theory of bone adaptation.
The key insight: bone responds only to loads that exceed its habitual threshold. Walking every day is good for general health, but because your bones are adapted to that level of stress, it produces little additional bone formation. Novel, higher-intensity stimuli trigger the most adaptation, which is why resistance training and impact exercise outperform walking for BMD gains.
Hormonal and Molecular Pathways
A 2025 review in Frontiers in Physiology by Zheng and colleagues detailed several mechanisms through which exercise protects bone in older women:
Sclerostin suppression: Exercise reduces sclerostin, a protein that inhibits bone formation. Lower sclerostin = more osteoblast activity.
IGF-1 and growth hormone: Resistance and high-impact exercise stimulate growth factors that promote bone cell proliferation.
Improved calcium absorption: Regular weight-bearing exercise enhances the body's ability to absorb and utilize calcium in bone tissue.
Reduced bone turnover markers: Exercise can shift the ratio of bone resorption to formation markers favorably within weeks of starting a program.
Muscle-bone crosstalk: Contracting muscles release myokines (including irisin and IL-6) that directly stimulate osteoblasts — a critical link between muscle strength and bone health.
Beyond BMD: The Full Bone-Health Picture
It's important to understand that BMD is not the only thing that matters. Bone quality — the microarchitectural integrity of the trabecular network — matters just as much. Exercise has been shown to improve bone geometry and structural strength even when BMD gains are modest. Additionally, by improving muscle strength, coordination, reaction time, and balance, exercise dramatically reduces the risk of falling — and it's falls, not weak bones alone, that cause most fractures.
How does exercise help osteoporosis? Exercise builds bone by applying mechanical stress that signals osteoblasts (bone-building cells) to increase activity. It also improves muscle strength, balance, and coordination to prevent falls, and stimulates hormones and proteins that favor bone formation over resorption.
3. The 6 Best Exercise Types for Osteoporosis
If you are managing osteoporosis, you’ve likely been told to "stay active." But a landmark 2026 network meta-analysis by Lu and colleagues reveals that not all exercise types provide equal benefits for bone mineral density (BMD), balance, pain relief, and overall quality of life.
To build stronger bones and prevent fractures, you need a targeted strategy. Here is what the latest clinical evidence says about the six major exercise categories for osteoporosis.
Top-Rated Bone Builders (Maximum BMD Impact)
1. Resistance Training (Weight Lifting)
What it is: Lifting weights, using resistance bands, and performing progressive body-weight exercises.
How it works: Muscle contraction pulls on the tendons, creating a mechanical force that directly stimulates bone-remodelling cells.
The Evidence: Multiple meta-analyses confirm that structured resistance training significantly increases BMD in both the lumbar spine and femoral neck (hip) in postmenopausal women.
2. High-Impact Training
What it is: Jumping, skipping, plyometrics, and weight-bearing sports.
How it works: Impact forces create a rapid "shock" to the skeleton, which provides the maximum osteogenic (bone-building) stimulus.
The Evidence: Randomized controlled trials (such as the Basat RCT) show a significant increase in lumbar spine and femoral neck BMD when high-impact training is compared to standard strength training or control groups.
Strong Evidence (Best for Fall Prevention)
3. Balance & Proprioception Training
What it is: Single-leg stands, wobble boards, and stability drills.
How it works: Instead of building bone directly, balance training targets the #1 modifier of fracture risk: preventing the fall in the first place.
The Evidence: Strongly endorsed by the Bae et al. position statement, dedicated balance training reduces overall fall risk by up to 40%.
4. Tai Chi
What it is: A mind-body practice combining slow, deliberate movements, dynamic weight shifting, and focused breathing.
How it works: It enhances functional lower-body strength, coordination, and spatial awareness.
The Evidence: Multiple RCTs demonstrate that Tai Chi simultaneously decreases fall rates while improving BMD, balance, and psychological quality of life.
Good & Supportive Evidence (Best for Mobility & Pain)
5. Pilates
What it is: Mat or reformer-based exercises focusing on core strengthening, postural correction, and body awareness.
The Evidence: According to the Angin RCT, Pilates leads to significant improvements in BMD, physical performance, and quality of life (QoL) in postmenopausal women, making it excellent for postural alignment.
6. Aquatic Exercise (Pool-Based Workouts)
What it is: Water aerobics, swimming, or water walking.
The Evidence: Because water buoyancy reduces gravity's impact, aquatic exercise offers a lower direct BMD stimulus. However, it ranks highest for pain relief and quality of life.
Who it's for: This is an ideal starting point or adjunct therapy for highly deconditioned patients, or those with severe fracture risks and chronic joint pain.
Why Walking is Helpful, But Not Enough Alone
Walking is the most frequently recommended exercise for bone health—but the data shows a gap between popular advice and clinical reality.
A comprehensive review by Pinheiro and colleagues found that while walking provides modest benefits for cardiovascular health and lumbar BMD, it is insufficient as a standalone bone-building strategy.
The Takeaway: Walk for your heart, but lift and jump for your bones. Programs that combine multiple exercise types (multimodal training) show far greater effectiveness than walking alone.
What About Vibration Therapy (WBV)?
Whole-body vibration (WBV) platforms have surged in popularity, but do they work?
The current evidence is mixed. While some studies show modest BMD benefits—particularly for sedentary or frail individuals who cannot perform traditional workouts—WBV should be viewed as a supplemental tool, not a replacement for active movement. For the best results, it should be combined directly with a resistance training routine
.
4. HiRIT — The Gold-Standard Combined Protocol
Key Finding According to a 2024 narrative review published in the International Journal of Sports and Exercise Medicine (Mathew, Zumwalt, Khemka), combined exercise protocols — particularly high-intensity resistance and impact training (HiRIT) — appear to be the most effective interventions for osteoporosis management in postmenopausal women.
HiRIT combines two powerful osteogenic stimuli:
Heavy resistance training — loading the skeleton with significant mechanical force through the pull of contracting muscles
High-impact activities — ground-reaction forces from jumping and dynamic movement
The LIFTMOR trial — one of the most cited RCTs on this topic — demonstrated that supervised, high-intensity resistance and impact training produced significantly greater improvements in lumbar spine and femoral neck BMD compared to low-intensity exercise, without increased injury rates when properly supervised.
⚠ Important: HiRIT Requires Supervision
High-intensity protocols carry injury risk if performed with poor form, excessive load, or without professional assessment. These programs should be designed and initially supervised by a physiotherapist, certified exercise physiologist, or trained fitness professional with experience in osteoporosis management. Always get medical clearance first.
Understanding the LIFTMOR Protocol: High-Intensity Training for Osteoporosis
When it comes to reversing bone loss, gentle exercises like walking often fall short. Enter the LIFTMOR Protocol (Lifting Intervention For Training Muscle and Osteoporosis Rehabilitation).
This groundbreaking, evidence-based exercise framework shattered traditional beliefs by proving that heavy, supervised weight training is not only safe for individuals with low bone mass but highly effective at increasing bone mineral density (BMD) and reducing fracture risks.
Here is a breakdown of the core elements that make up the LIFTMOR protocol.
The LIFTMOR Exercise Routine & Layout
The protocol is highly structured, focusing on low repetitions, high weights, and explosive impact movements. It is performed 2 times per week under strict, qualified supervision.
1. The Core Resistance Exercises
To stimulate bone growth in the most fracture-prone areas (like the spine and hips), the program utilizes compound barbell movements.
Deadlifts (5 sets × 5 repetitions)
Overhead Presses (5 sets × 5 repetitions)
Back Squats (5 sets × 5 repetitions)
2. The Intensity Level
85%+ of 1RM (One-Repetition Maximum): Participants lift heavy. The load is calculated so that the 5th repetition feels highly challenging, directly triggering the mechanical stress required for bone remodeling.
3. The Impact Component
Drop Jumps (3 sets × 10 repetitions): Participants step off a small box and land firmly, executing a maximal effort impact to shock the skeletal system and stimulate bone density.
Frequency: 2 times per week, strictly supervised
Vital Safety Note
The LIFTMOR protocol is not a do-it-yourself gym routine. Because it involves lifting heavy loads near maximum capacity, it requires prior clearance from a physician and must be performed under the direct guidance of a qualified exercise physiologist or trainer specializing in bone health. Proper lifting form is mandatory to prevent injury and safely reap the bone-building rewards.
5 .Exercises to Avoid (and Safe Modifications) with Osteoporosis
When you are managing low bone density, knowing what movements to eliminate or modify is just as crucial as tracking down the right workout routine.
The spine—specifically your thoracic (mid-back) and lumbar (lower back) vertebrae—is statistically the most common fracture site in individuals with osteoporosis. To keep your skeleton protected during physical activity, prioritizing spinal alignment is a non-negotiable rule.
Why "Neutral Spine" Matters for Bone Safety
The main objective when modifying an exercise is avoiding excessive pressure on the front edge of your vertebrae. Rounded or hunched postures squeeze the front of your spinal bones, significantly rising the risk of a compression fracture.
Instead, look to build strength while holding a stable, straight back alignment.
Critical Rules: Movements to Avoid
Loaded Forward Bending (Flexion): Stop doing traditional sit-ups, abdominal crunches, and toe touches. Bending your spine forward places heavy compressive pressure on the front edge of your vertebrae, drastically increasing your risk of a spinal compression fracture.
Weighted Twisting (Rotation): Avoid seated twisting machines or aggressive torso rotations while holding weights. These movements create sharp shear forces across vulnerable spinal joints.
Unsupervised High Impact: Skip jumping, running, or skipping workouts if you have severe osteoporosis or a history of bone loss, unless you are under the direct supervision of a specialized clinician.
Slouched Rowing: Do not use rowing machines if your upper back rounds or hunches forward at the catch phase of the stroke.
Extreme Yoga & Flexibility Poses: Eliminate deep forward folds, plough poses, and spinal inversions (like headstands), which force your spine to bear your body weight while bent out of alignment.
High-Fall-Risk Recreation: Steer clear of sports with a high risk of hard tumbles, such as downhill skiing, ice skating, and rollerblading, where a single fall can result in an immediate hip or wrist fracture.
Smart Modifications: Safer Alternatives
Swap Crunches for Core Bracing: Protect your back by replacing sit-ups with the Plank, Bird-Dog, or Dead Bug exercises. These movements build deep abdominal strength while keeping your spine completely flat and safe.
Modify Your Rowing Technique: If you use cable machines or dumbbells for rows, focus on keeping your chest proud and your torso strictly upright and braced.
Choose Lower-Impact Cardio: Trade high-risk sports for Nordic walking with stability poles or riding a stationary bicycle to safely work your cardiovascular system without the fear of falling.
Opt for Gentle Mind-Body Practices: Trade intense, hyper-flexible yoga routines for Chair Yoga or modified, neutral-spine Tai Chi movements that focus on stability and balance.
Special Safety Advisory
The Golden Rule: Always prioritize a neutral spine (keeping your back straight and tall) over slouched or rounded postures during all daily activities and workouts.
Past Fractures Change the Rules: If you have already suffered a vertebral compression fracture, you must work exclusively with a physical therapist. Do not attempt any high-intensity lifting or high-impact protocols without explicit medical clearance.
6. Sample Workout Plans by Fitness Level
The following programs are based on the exercise prescriptions reviewed in position statements from the Journal of Bone Metabolism (Bae et al., 2023) and synthesized from the 2026 meta-analyses. Adapt to your ability and always progress gradually.
Beginner Plan — Weeks 1–8 (3× per week)
For those new to exercise or with significant deconditioning. Focus: safety, body awareness, and laying the foundation.
Warm-up (5 min): March in place, arm circles, gentle hip circles
Chair sit-to-stand — 3 sets × 10 reps (teaches squat mechanics safely)
Wall push-ups — 3 sets × 10 reps
Hip hinge/deadlift pattern with dowel rod — 3 sets × 10 reps (form focus)
Resistance band rows — 3 sets × 12 reps (upright posture)
Single-leg balance (holding chair) — 3 × 20 seconds each side
Heel drops — 3 sets × 10 (mild impact stimulus, bone stimulus at hip)
Cool-down: 5 min gentle walking + hip flexor stretch
Intermediate Plan — Weeks 9–24 (3× per week)
For those with 2+ months of exercise base. Focus: progressive resistance, structured impact, balance challenge.
Warm-up (5–8 min): Brisk walk, dynamic hip swings, bodyweight squats × 10
Goblet squat (dumbbell) — 4 sets × 8–10 reps at moderate load
Romanian deadlift (dumbbells) — 4 sets × 8 reps
Dumbbell shoulder press — 3 sets × 10 reps
Resistance band or cable rows — 3 sets × 10–12 reps
Step-ups (onto a sturdy step) — 3 sets × 10 each leg
Box jumps / jump squats (if medically cleared) — 3 sets × 5–8 reps
Balance: tandem stance + perturbation — 3 × 30 sec each side
Pilates-style core: bird-dog, dead bug — 2 × 10 each
Advanced / HiRIT-Style Plan (2× per week, supervised)
For those with solid training history, medical clearance, and professional supervision. Closely follows evidence-based HiRIT structure.
Deadlift — 5 sets × 5 reps at ≥80% 1RM
Back squat or trap-bar squat — 5 sets × 5 reps at ≥80% 1RM
Overhead press — 5 sets × 5 reps at ≥80% 1RM
Weighted chin-up or lat pulldown — 3 sets × 6–8 reps
Drop jumps / box jumps — 3 sets × 8–10 reps, maximal effort
Single-leg hop & stick — 3 × 6 each leg (proprioception + impact)
Rest: 3 min between heavy sets
⚠ Progressive overload is essential: increase weight by 2–5% when you can complete all reps with good form across two consecutive sessions.
The Role of Mind-Body Exercise: Tai Chi & Pilates
Tai Chi and Pilates serve a complementary role that goes beyond BMD numbers. Both are supported by RCT evidence for reducing falls, improving balance, reducing pain, and improving quality of life in osteoporosis patients. They are particularly valuable for:
Individuals with significant pain or fear of exercise (kinesiophobia)
Early rehabilitation after fracture or surgery
Older adults who are not candidates for high-intensity programs
Anyone wanting a twice-weekly complement to their strength training
Aim for at least 2 sessions of Tai Chi or Pilates per week as an adjunct to resistance training for the most comprehensive benefit.
7. Evidence Summary: What the Research Shows
Skeletal Health Scorecard: Exercise Type Comparison
HiRIT (Combined High-Intensity Resistance and Impact): ⭐⭐⭐⭐⭐
Best For: Overall effectiveness, balancing high BMD gains with superior fall prevention.
Evidence: High (backed by RCTs and meta-analyses).
Resistance Training: ⭐⭐⭐⭐
Best For: Strong, consistent Bone Mineral Density (BMD) gains and increasing muscle mass.
Evidence: High.
High-Impact Exercise (Jumping): ⭐⭐⭐⭐
Best For: Maximizing spinal and hip BMD gains through mechanical loading.
Evidence: Moderate–High.
Tai Chi: ⭐⭐⭐⭐
Best For: Exceptional fall prevention and improving dynamic balance; excellent for QoL.
Evidence: Moderate–High.
Pilates: ⭐⭐⭐
Best For: Postural alignment, core strength, and quality of life.
Evidence: Moderate.
Walking: ⭐⭐
Best For: General cardiovascular health; modest benefit for lumbar BMD only. Insufficient as a standalone bone builder.
Evidence: Moderate.
Aquatic Exercise: ⭐⭐
Best For: Superior pain relief and mobility in high-risk patients; limited direct BMD impact.
Evidence: Moderate.
Whole-Body Vibration (WBV): ⭐
Best For: Frail or sedentary populations (limited applications).
Evidence: Low–Moderate.
(Note: Grading system: ★ = minimal evidence/effect; ★★★★★ = strong evidence of consistent benefit. Based on data from Lu et al. 2026, Alnasser et al. 2025, Mathew et al. 2024, and Zou & Liu 2026.)
The Bone Building Timeline: How Long Until Results?
Bone Remodeling (The Slow Gain): Remember, strengthening bone is slow. Measurable changes in your structural Bone Mineral Density (BMD) typically take 12 to 24 months of consistent, optimized training.
Bone Turnover Markers (The Early Indicators): Blood and urine biomarkers of bone formation can detect positive changes in your body's bone-building activity as early as 6 to 12 weeks.
Functional Gains (The Immediate Wins): You will see results much faster in other areas. Significant improvements in muscle strength, balance, and physical performance begin within just 4 to 8 weeks. Because these functional gains reduce the immediate risk of falls (which cause fractures), these early changes matter enormously for your safety.
8. Common Myths & Mistakes About Exercise and Osteoporosis
❌ Myth #1
"Exercise is dangerous if you have osteoporosis — you'll fracture a bone."
✅ The Truth: When properly prescribed and supervised, exercise is safe and beneficial for virtually everyone with osteoporosis. Inactivity is far more dangerous in the long run: sedentary people lose bone and muscle simultaneously, increasing both fracture risk and fall risk. The key is starting at an appropriate intensity and building progressively.
❌ Myth #2
"Walking every day is enough to protect my bones."
✅ The Truth:Walking provides modest benefits but is insufficient as a standalone strategy for anyone already diagnosed with osteopenia or osteoporosis. Bone needs novel mechanical loading above its habitual threshold. Resistance training and impact exercise are essential additions.
❌ Myth #3
"I'm too old or too frail to lift heavy weights."
✅ The Truth:Age is not a disqualifier from resistance training. Clinical trials have included women in their 70s and 80s performing supervised heavy resistance training with excellent results and minimal injury risk. The dose (weight, intensity) is always adjusted to the individual — but the stimulus must still exceed the habitual threshold to be effective.
❌ Myth #4
"Calcium supplements alone will protect my bone health without exercise."
✅ The Truth:Calcium and Vitamin D are essential supporting nutrients, but they cannot substitute for the mechanical stimulus of exercise. Without loading, bones have little reason to incorporate available calcium into new tissue. Exercise and nutrition work synergistically — you need both.
❌ Myth #5
"Swimming is the best exercise because it's easy on the joints."
✅ The Truth:While swimming is excellent for cardiovascular health, joint mobility, and pain relief, it provides minimal mechanical loading on bones due to buoyancy. It ranks lowest for BMD improvement among common exercise types. Use it as a complement, not a replacement, for weight-bearing and resistance exercise.
9.Medical Context: Merging Exercise with Osteoporosis Medications
Exercise provides the mechanical signal to build bone, but high-risk patients need the biological support of medication to maximize those results.
The Integrated T-Score Blueprint
Mild Bone Loss (Osteopenia | T-score -1.0 to -2.5):
The Strategy: Exercise-First Approach.
How it works: Progressive resistance training, active impact drills, and lifestyle adjustments are often sufficient as primary therapies to stimulate bone remodeling and prevent progression to osteoporosis.
Established Osteoporosis (T-score -2.5 to -3.5 OR prior fracture):
The Strategy: Antiresorptive Medications + Strength Training.
How it works: Medications like Bisphosphonates (e.g., alendronate) or RANKL inhibitors (e.g., denosumab) slow down bone breakdown cells (osteoclasts). Performing progressive weight training simultaneously signals your bone-building cells (osteoblasts) to lock in and strengthen the remaining bone matrix.
Severe/Advanced Osteoporosis (T-score lower than -3.5 OR multiple spinal fractures):
The Strategy: Anabolic Agents + Supervised Training (HiRIT).
How it works: Bone-building medications like Parathyroid Hormone analogs (e.g., teriparatide) or Sclerostin inhibitors (e.g., romosozumab) actively accelerate new bone formation. Pairing these anabolic drugs with high-intensity protocols like LIFTMOR creates a powerful synergistic effect—the medication chemically activates the bone cells, while the heavy lifting mechanically directs that new bone layout precisely where the skeleton needs it most (the spine and hips).
Clinical Takeaway for Patients: Think of medication as the raw materials delivered to a construction site, and progressive exercise as the building crew. Medication alters your systemic bone chemistry, but mechanical loading determines exactly where and how effectively that bone is structured.
10 Frequently Asked Questions
What is the single best exercise for osteoporosis?
No single exercise is definitively "best" — the strongest evidence supports combined protocols that pair resistance training with high-impact exercise (HiRIT). If you can only do one thing, progressive resistance training (weightlifting) has the most robust and consistent evidence for improving bone mineral density at the lumbar spine and femoral neck, while simultaneously reducing fall risk.
Can exercise reverse osteoporosis, or only slow it down?
Exercise can produce modest but clinically meaningful increases in bone mineral density (typically 1–8% depending on the site, program, and individual) and can reverse osteopenia in some cases. For established osteoporosis, the primary goal shifts toward slowing further bone loss, improving bone quality, building muscle, and preventing falls — all of which exercise accomplishes effectively. Exercise is almost always used alongside medication (bisphosphonates, etc.) for moderate-to-severe osteoporosis.
How often should someone with osteoporosis exercise?
The 2023 position statement from the Journal of Bone Metabolism (Bae et al.) and multiple clinical guidelines recommend:
Resistance training: 2–3 times per week with at least one rest day between sessions
Balance training: Daily or near-daily practice (even brief sessions of 10–15 minutes are beneficial)
Aerobic weight-bearing activity: 150+ minutes per week (e.g., brisk walking, stair climbing)
Flexibility/mind-body (Tai Chi, Pilates): 2–3 times per week
Is yoga safe for osteoporosis?
Yoga can be safe and beneficial with modifications — but standard classes may include poses that are risky for osteoporotic spines. Avoid deep forward folds, spinal twists under load, and inversions. Look for instructors specifically trained in osteoporosis-adapted yoga, or try chair yoga. The balance, body awareness, and strength elements of yoga are genuinely helpful when practised safely.
What exercises improve bone density in the hips?
The hip (specifically the femoral neck) responds best to exercises that load it directly: squats, deadlifts, lunges, step-ups, and jumping exercises (when appropriate). Closed-chain exercises — where your foot is in contact with a surface — appear more effective for hip BMD than open-chain exercises. A 2024 narrative review confirms that resistance training and high-impact protocols produce the most significant femoral neck BMD gains.
What exercises improve bone density in the spine?
Lumbar spine BMD responds particularly well to axial loading exercises — those that load the spine in compression: squats, deadlifts, overhead presses, and walking with a loaded pack (carefully). Pilates and Clinical Pilates exercises have also shown significant lumbar spine BMD improvements in RCTs. Avoid spinal flexion under load (like sit-ups) which increases fracture risk at the anterior vertebral body.
Is it safe to exercise after a vertebral fracture?
Yes, but only with professional guidance. After the acute phase of a vertebral compression fracture, carefully selected exercises — focusing on gentle spinal extension, postural muscles, and lower-limb strengthening — can aid recovery and prevent future fractures. Work with a physiotherapist who specializes in osteoporosis. Avoid all spinal flexion and twisting movements during recovery.
Can exercise help with osteoporosis pain?
Yes. Multiple studies show that exercise significantly reduces chronic musculoskeletal pain associated with osteoporosis. Aquatic exercise, Pilates, and Tai Chi showed the strongest pain-relief effects in clinical reviews. Improved posture, core strength, and muscle support around the spine reduce compression-related pain. The 2026 network meta-analysis by Lu et al. confirmed pain improvement as a consistent benefit across exercise modalities.
Should I take calcium and vitamin D supplements if I exercise for bone health?
Nutrition and exercise work synergistically. Most adults over 50 benefit from ensuring adequate calcium (1,000–1,200 mg/day from food and supplements combined) and vitamin D (1,000–2,000 IU/day depending on bloodwork). Exercise creates the demand; nutrients provide the raw materials for bone formation. Discuss supplementation with your doctor — your needs depend on diet, sun exposure, bloodwork, and medications.
What is the difference between osteopenia and osteoporosis exercise guidelines?
The exercise principles are largely the same for both conditions, but the starting point and progression differ. People with osteopenia generally have more capacity for impact and loading, and have a larger window for true prevention. Those with established osteoporosis — especially with prior fractures — need more conservative starting points, closer supervision, and more individualized modifications. The 2026 Lu et al. meta-analysis confirmed that exercise improves outcomes in both groups.
How does exercise compare to medication (bisphosphonates) for osteoporosis?
Exercise and medication are not competing approaches — they are complementary. Bisphosphonates and other bone medications primarily work by slowing bone resorption; exercise stimulates bone formation and builds the muscle and balance that medications cannot address. For moderate-to-severe osteoporosis, clinical guidelines recommend both simultaneously. Exercise alone may be sufficient for osteopenia or low-risk cases; that determination belongs to your physician.
10. Conclusion & Action Steps
The science on exercise for osteoporosis is clear and increasingly compelling: the right exercise program, consistently applied, is one of the most powerful interventions available for bone health — and it works at any age. Here is what the evidence tells us:
Combined protocols work best. Pairing resistance training with high-impact exercise (HiRIT) produces the largest BMD gains. Don't choose one to the exclusion of the other.
Resistance training is non-negotiable. For bone-building purposes, lifting weights (or equivalent) 2–3 times per week is the single most evidence-backed practice.
Falls prevention is just as important as BMD. Balance training, Tai Chi, and Pilates reduce fracture risk by preventing falls — arguably the most important outcome metric.
Walking is a foundation, not a solution. It's good for health, but insufficient for bone-building. You need to add load and impact.
Some movements need to be avoided. Spinal flexion under load is particularly dangerous — swap crunches for planks and bird-dogs.
Consistency over intensity. A moderate program sustained for 12–24 months will outperform an intense program abandoned after 8 weeks.
Your 5-Step Action Plan — Start This Week
You don't need a gym membership or expensive equipment to begin protecting your bones today.
✅ Step 1: Get a DEXA scan if you haven't had one — know your T-score baseline
✅ Step 2: Speak with your doctor about your fracture risk and any exercise restrictions
✅ Step 3: Begin the Beginner workout plan above, or book a session with a physiotherapist to get a personalized program
✅ Step 4: Add 10 minutes of balance practice daily — start with single-leg stands while brushing your teeth
✅ Step 5: Review your calcium and vitamin D intake with your doctor and adjust as needed
This information is for educational purposes only and should not replace professional medical advice. Always consult with your healthcare provider for personalized recommendations based on your individual health status and risk factors.
Related Articles
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | DR T S DIDWAL
References
Alnasser, S. M., Babakair, R. A., Al Mukhlid, A. F., et al. (2025). Effectiveness of exercise loading on bone mineral density and quality of life among people diagnosed with osteoporosis, osteopenia, and at risk of osteoporosis: A systematic review and meta-analysis. Journal of Clinical Medicine, 14(12), 4109. https://doi.org/10.3390/jcm14124109
Angin, E., Erden, Z., & Can, F. (2015). The effects of clinical Pilates exercises on bone mineral density, physical performance and quality of life of women with postmenopausal osteoporosis. Journal of Back and Musculoskeletal Rehabilitation, 28(4), 849–858.
Bae, S., Lee, S., Park, H., et al. (2023). Position statement: Exercise guidelines for osteoporosis management and fall prevention in osteoporosis patients. Journal of Bone Metabolism, 30(2), 149–165. https://doi.org/10.11005/jbm.2023.30.2.149
Basat, H., Esmaeilzadeh, S., & Yildiz, M. (2013). Preventive effects of combined exercise on bone mineral density in postmenopausal women. Journal of Back and Musculoskeletal Rehabilitation, 26(3), 311–318.
Benedetti, M. G., Furlini, G., Zati, A., & Letizia Mauro, G. (2018). The effectiveness of physical exercise on bone density in osteoporotic patients. BioMed Research International, 2018, Article 4840531. https://doi.org/10.1155/2018/4840531
Hong, A. R., & Kim, S. W. (2018). Effects of resistance exercise on bone health. Endocrinology and Metabolism, 33(4), 435–444. https://doi.org/10.3803/EnM.2018.33.4.435
Kelley, G. A., Kelley, K. S., & Tran, Z. V. (2001). Resistance training and bone mineral density in women: A meta-analysis of controlled trials. American Journal of Physical Medicine & Rehabilitation, 80(1), 65–77.
Koshy, J., Delpisheh, A., & Brabin, B. J. (2022). High-impact exercise and bone density in postmenopausal women: A systematic review.
Lu, Y. M., Zhang, S. W., Wang, Z. Z., et al. (2026). Comparative effectiveness of exercise interventions on bone mineral density, balance, pain, and quality of life in patients with osteopenia and osteoporosis: A systematic review and network meta-analysis. Discover Public Health, 23, 668. https://doi.org/10.1186/s12982-026-01949-4
Massini, D. A., et al. (2022). Evidence on the effects of exercise type and load on bone metabolism. International Journal of Environmental Research and Public Health, 19(15), 9466. https://doi.org/10.3390/ijerph19159466
Mathew, M., Zumwalt, M., & Khemka, S. (2024). Role of exercise in prevention and treatment of osteoporosis: A narrative review. International Journal of Sports and Exercise Medicine, 10, 269. https://doi.org/10.23937/2469-5718/1510269
National Osteoporosis Foundation. (2023). Clinician’s guide to prevention and treatment of osteoporosis. https://www.bonehealthandosteoporosis.org
Pinheiro, M. B., Oliveira, J. S., Bauman, A., et al. (2020). Evidence on physical activity and osteoporosis prevention for people aged 65 and older: Systematic review to inform the WHO guidelines. British Journal of Sports Medicine, 54(24), 1445–1452. https://doi.org/10.1136/bjsports-2020-102505
Sherrington, C., Fairhall, N. J., Wallbank, G. K., et al. (2019). Exercise for preventing falls in older people living in the community. Cochrane Database of Systematic Reviews, 2019(1), CD012424. https://doi.org/10.1002/14651858.CD012424.pub2
Shojaa, M., von Stengel, S., Kohl, M., et al. (2020). Effect of exercise training on bone mineral density in postmenopausal women: A systematic review and meta-analysis of intervention studies. Osteoporosis International, 31(1), 39–59. https://doi.org/10.1007/s00198-019-05103-2
Thabet, A. A., & Alshehri, M. A. (2016). Efficacy of deep core stability exercise program in postpartum lumbopelvic pain. Journal of Back and Musculoskeletal Rehabilitation, 29(3), 563–573.
Watson, S. L., Weeks, B. K., Weis, L. J., et al. (2018). High-intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopenia and osteoporosis: The LIFTMOR randomized controlled trial. Journal of Bone and Mineral Research, 33(2), 211–220. https://doi.org/10.1002/jbmr.3284
World Health Organization. (2022). Global report on falls prevention in older age. WHO Press.
Zheng, B., Chen, J., & Li, Y. (2025). Recent advances in the mechanisms and rehabilitation strategies of exercise interventions for osteoporosis in older adult women. Frontiers in Physiology, 16, 1631817. https://doi.org/10.3389/fphys.2025.1631817
Zou, W., & Liu, R. (2026). Diverse exercise modalities in alleviating osteoporosis: A narrative review. Endocrine, 91(1), 66–78. https://doi.org/10.1007/s12020-026-04551-5
Editorial Note on Sources
This article synthesizes evidence from peer-reviewed systematic reviews, randomized controlled trials, network meta-analyses, narrative reviews, and clinical position statements published primarily between 2023 and 2026. Where limitations existed — including small sample sizes, heterogeneous exercise protocols, or short intervention durations — these limitations were acknowledged contextually. All recommendations are intended for general educational purposes and should not replace individualized medical advice from a qualified healthcare professional.