The Fat Inside Your Muscles: More Dangerous Than We Thought?
Muscle quality matters more than muscle size. Learn how hidden muscle fat impacts insulin sensitivity, recovery, inflammation, and healthy aging in this evidence-based guide.
EXERCISEMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/15/202615 min read
For decades, we believed muscle weakness was mostly a problem of aging, inactivity, or simply “losing muscle mass.” But modern metabolic science is revealing a far more complex — and far more concerning — reality. In many people, the real issue is not just a shrinking muscle. It is fat quietly infiltrating the muscle itself.
This hidden phenomenon, known as intramuscular fat accumulation, is now emerging as a major driver of insulin resistance, metabolic dysfunction, sarcopenia, frailty, poor exercise recovery, and chronic inflammation (Razi et al., 2025). Unlike the fat you can see around the waist or under the skin, this “stealth fat” hides deep inside skeletal muscle tissue, disrupting the very systems responsible for strength, mobility, glucose control, and healthy aging.
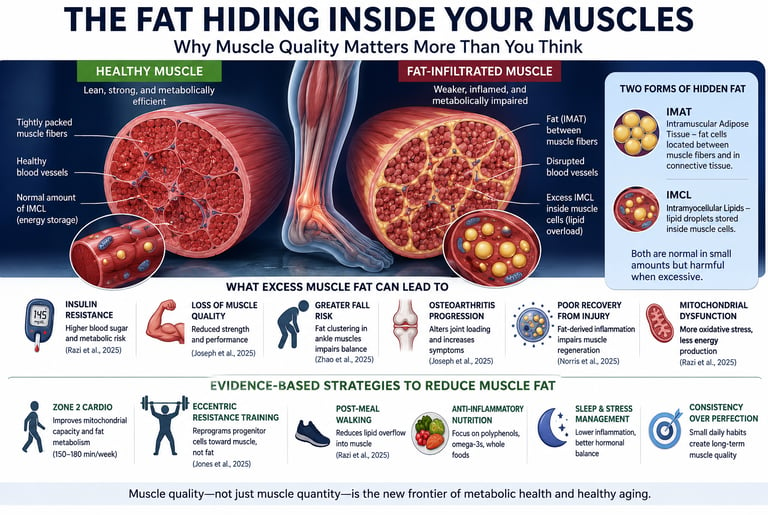
Researchers describe two major forms of this hidden fat: intramuscular adipose tissue (IMAT), which accumulates between muscle fibers, and intramyocellular lipids (IMCL), tiny fat droplets stored inside muscle cells themselves. In healthy, physically active individuals, small amounts of IMCL can serve as an efficient energy reserve. But in sedentary or metabolically unhealthy states, these lipids can become biologically toxic, triggering inflammation, mitochondrial dysfunction, oxidative stress, and impaired insulin signaling (Jones et al., 2025; Razi et al., 2025).
What makes this discovery especially important is that intramuscular fat appears to predict far more than body weight alone. Studies now link elevated muscle fat infiltration with reduced muscle quality, slower recovery after injury, increased fall risk, osteoarthritis progression, and declining metabolic flexibility (Norris et al., 2025; Zhao et al., 2025). In other words, two people may have the same amount of muscle on a scan — yet one may possess metabolically resilient tissue, while the other carries muscle increasingly compromised by hidden fat deposition.
The encouraging news is that this process is not irreversible. Emerging evidence shows that targeted exercise, anti-inflammatory nutrition, mitochondrial conditioning, and improved metabolic health can help remodel muscle tissue from the inside out.
What Exactly Is Intramuscular Fat?
The term covers two related but distinct phenomena.
IMAT refers to actual fat cells (adipocytes) that take up residence between muscle fibres and in the connective tissue compartments of skeletal muscle. On an MRI scan, it appears as white streaks threading through what should be uniformly dense muscle tissue — think of the marbling you see in a fatty cut of steak. This is not fat that simply surrounds the muscle; it is fat within the muscle architecture itself.
IMCL is subtler still: these are lipid droplets stored inside individual muscle cells. Rather than being a separate cell type, IMCL represents fat stored within the very contractile units that power your every movement.
Both forms are normal in small quantities. But when they accumulate beyond healthy thresholds — driven by aging, obesity, inactivity, or chronic inflammation — they shift from benign energy reserves to active disruptors of muscle function and metabolism.
Where Does This Fat Come From? The Cellular Story
To understand intramuscular fat, you need to meet a group of cells most people have never heard of: fibro-adipogenic progenitor cells, or FAPs.
FAPs are resident stem-like cells living inside skeletal muscle. Under healthy conditions, they act as quiet support staff — helping coordinate repair after injury and maintaining the structural scaffolding of muscle tissue. But FAPs have a dual identity. Depending on the signals they receive from their environment, they can either support muscle regeneration or transform into fat-storing adipocytes.
Jones, Kopinke, and Meyer (2025) provided a detailed mechanistic map of this process. When muscles are chronically inflamed, when aging degrades the regulatory signals from immune cells and satellite cells (the muscle's primary repair stem cells), or when metabolic disease disrupts the cellular microenvironment, FAPs receive the wrong instructions. They pivot toward fat production, progressively replacing functional muscle with adipose tissue.
Key signals in this process include macrophage-derived inflammatory molecules, transforming growth factor-beta (TGF-β), and hedgehog pathway activity. In youth and good health, these signals keep FAPs in a repair-supportive mode. In aging, obesity, and chronic inflammation, the balance tips — and the FAP "switch" flips toward fat.
This explains why intramuscular fat accumulation is not random. It is the product of a regulated but misdirected biological programme — and one that, in principle, can be therapeutically redirected.
The Vascular Angle: New Evidence From 2026
One of the most illuminating recent discoveries comes from a 2026 Nature Metabolism study by AlZaim and colleagues, who mapped the vascular niche of human adipose tissue across different metabolic states. Their work revealed that the blood vessel environment within and around fat depots — including those adjacent to muscle — differs significantly depending on whether a person is metabolically healthy or not.
In metabolically compromised individuals, the vascular architecture supporting adipose tissue becomes altered in ways that promote inflammatory signalling and impair the crosstalk between fat cells and surrounding muscle fibres (AlZaim et al., 2026). This finding reframes intramuscular fat not just as a cellular problem, but as a vascular one: the microenvironment that feeds and sustains this fat is itself in a pathological state in people with obesity or metabolic syndrome, creating conditions that perpetuate fat infiltration and resist clearance.
This vascular dimension also helps explain why simply losing weight does not always promptly resolve intramuscular fat accumulation — the tissue environment itself may need to be rehabilitated.
Mapping the Damage: Where Fat Clusters Are and Why It Matters
Not all intramuscular fat is equally placed or equally dangerous. Location matters enormously.
Zhao and colleagues (2025) used advanced MRI-based spatial mapping to study fat distribution within the ankle plantar flexor muscles — the group responsible for pushing off the ground when you walk, climb stairs, or recover your balance after a stumble. Their critical finding was that intramuscular fat in older adults does not spread uniformly across the muscle. Instead, it clusters in specific fascicles and connective tissue compartments.
This spatial pattern is more than an imaging curiosity. Because muscle force transmission depends on the coordinated activation of precise fibre groups, fat clustering in particular regions can selectively impair the rapid, coordinated contractions needed for balance correction — even when total muscle volume appears adequate. In practical terms, an older adult may have seemingly sufficient leg muscle mass yet still be at elevated fall risk because the quality of key muscle compartments has been silently eroded by fat infiltration.
Meanwhile, Joseph et al (2025) applied a similar MRI methodology to a far larger scale. Using data from the Osteoarthritis Initiative — a cohort of over 4,000 adults aged 45 to 79 — they quantified thigh intramuscular fat across thousands of participants and identified clear associations with age, sex, and body mass index (BMI). Women and men showed different spatial patterns of fat infiltration even when total volumes were comparable, with implications for understanding sex-based differences in knee osteoarthritis risk and severity.
Critically, BMI predicted IMAT independently of age — but the relationship was not perfectly linear, suggesting that metabolic factors beyond simple adiposity (such as insulin sensitivity and inflammation status) influence how much fat infiltrates muscle tissue.
Fat as an Active Saboteur: The Recovery Connection
Perhaps the most alarming finding in recent intramuscular fat research is the shift in understanding its role in muscle recovery. For years, elevated IMAT was seen as a marker of poor recovery — a sign that things had gone wrong. A landmark 2025 study by Norris and colleagues overturned that passive interpretation.
Using mouse genetic models and pharmacological tools to selectively induce IMAT accumulation, the researchers found that muscles with elevated intramuscular fat showed significantly impaired regeneration after standardised injury — across metrics including maximal force production, muscle fibre cross-sectional area, and satellite cell activation. Crucially, the adipocytes within the muscle were not merely taking up space. They were actively secreting inflammatory factors that suppressed regenerative signalling and remodelled the extracellular matrix in ways that made fibre repair less efficient (Norris et al., 2025).
This finding has immediate clinical implications. Patients recovering from orthopaedic surgery, traumatic muscle injury, or prolonged immobilisation who carry pre-existing IMAT may face a systematically compromised healing trajectory — not because their rehabilitation programme is inadequate, but because the tissue environment itself is hostile to repair. The implication is provocative: reducing intramuscular fat may need to become a prehabilitation objective, addressed before recovery-critical interventions, not just during them.
The Regeneration Paradox: Fat as Friend and Foe
Complicating the picture further, a 2026 review by Lu, Lu, and Cai in the Journal of Cachexia, Sarcopenia and Muscle highlighted what the authors describe as the dual roles of adipose tissue in skeletal muscle regeneration. In the early phases of muscle injury, adipose-derived cells and signals can actually support the inflammatory and clean-up phase that precedes repair — acting as a pro-regenerative partner. However, when fat accumulation is excessive or chronically sustained, the same tissue transitions into a maladaptive state that interferes with the later phases of regeneration (Lu et al., 2026).
This temporal nuance is important for clinical practice. It suggests that the goal is not the elimination of all intramuscular lipid but the right amount in the right compartment at the right time — a concept the authors frame as metabolic and regenerative flexibility. An acute injury in someone with low baseline IMAT may benefit from some local adipose-derived signalling; the same injury in someone with chronically high IMAT is likely to be impaired by the same signals turning maladaptive.
The Obesity–Insulin Resistance Pipeline Runs Through Your Muscles
For people living with obesity or prediabetes, intramuscular fat is not a peripheral concern — it is central to the disease mechanism.
Razi and colleagues (2025) provided one of the most comprehensive mechanistic reviews of how intramyocellular lipids (IMCL) mediate insulin resistance in skeletal muscle. Their analysis identifies three parallel pathways through which excess IMCL disrupts insulin signalling:
Lipid overflow: When circulating fatty acids exceed the muscle's capacity for storage or oxidation, they accumulate as diacylglycerols (DAGs) and ceramides — bioactive intermediates that directly interfere with the insulin receptor signalling cascade.
Inflammatory kinase activation: Adipose-derived cytokines including TNF-α and IL-6 activate serine/threonine kinases (particularly JNK and IKKβ) that phosphorylate and inactivate key insulin signalling proteins.
Mitochondrial dysfunction and oxidative stress: Overwhelmed mitochondria generate reactive oxygen species (ROS) that further damage insulin signalling enzymes and impair the muscle's ability to clear glucose from the bloodstream.
The "athlete's paradox" — the observation that elite endurance athletes also have high IMCL yet are extraordinarily insulin sensitive — is explained by metabolic quality, not fat quantity. In trained athletes, lipid droplets are efficiently mobilised and oxidised during exercise, with minimal accumulation of the toxic intermediates that cause metabolic harm. In sedentary, obese individuals, the same fat sits stagnant, producing inflammation and blocking insulin action.
The clinical message: the goal is not zero muscle fat, but a metabolically flexible muscle that can burn what it stores.
Practical Applications: Your "Metabolic Clean-Up" Protocol
The science converges on a set of evidence-based strategies that target intramuscular fat through both mechanical and metabolic pathways. These are not exotic interventions — they are refinements of principles most people have heard before, now understood with greater mechanistic precision.
1. Zone 2 Cardio: Training Your Mitochondria
Low-intensity aerobic exercise — brisk walking, easy cycling, light swimming at a pace where you can still hold a conversation — is the most effective stimulus for improving mitochondrial oxidative capacity. This directly addresses the mitochondrial dysfunction that allows IMCL to accumulate into toxic intermediates. Aim for 150–180 minutes per week, distributed across most days.
2. Eccentric Resistance Training: Reprogramming FAPs
The slow, controlled "lowering" phase of resistance exercises — such as taking 3–4 seconds to lower yourself into a squat or slowly lowering a weight — generates a specific mechanical stimulus that activates satellite cells and appears to favour FAP differentiation toward muscle repair rather than fat storage. Two to three resistance sessions per week incorporating this eccentric emphasis are supported by the mechanistic literature.
3. The 10-Minute Post-Meal Walk
Even a short walk after meals helps clear circulating fatty acids and glucose before they can "overflow" into muscle tissue as excess lipid. This simple habit addresses the lipid oversupply pathway identified by Razi and colleagues (2025) and requires no gym equipment or significant time investment.
4. Ankle Plantar Flexor-Specific Exercises
Given the specific fat clustering identified in ankle muscles by Zhao and colleagues (2025) and its association with falls risk, targeted exercises for this muscle group deserve explicit attention. Calf raises — particularly single-leg variations and slow eccentric lowering — directly stress the plantar flexors. For older adults, this group should be a priority, not an afterthought.
5. Anti-Inflammatory Nutrition
Chronic low-grade inflammation is the environmental signal that flips FAPs from repair mode to fat-storage mode. A diet rich in polyphenols — berries, leafy greens, green tea, olive oil — provides antioxidants that counteract the oxidative stress and inflammatory kinase activation described by Razi and colleagues. Reducing ultra-processed foods, refined carbohydrates, and excess saturated fat lowers the systemic inflammatory burden that feeds IMAT accumulation.
6. Prioritise Sleep and Stress Management
Poor sleep and chronic psychological stress both elevate cortisol and systemic inflammatory markers — two drivers of the FAP dysregulation described by Jones and colleagues (2025). Seven to nine hours of quality sleep per night is not a luxury; in the context of muscle fat biology, it is a metabolic intervention.
7. Consider Your Prehabilitation Status
If you are planning orthopaedic surgery, expect a period of immobilisation, or are entering intensive rehabilitation, ask your healthcare provider about assessing your baseline muscle quality — not just muscle strength or mass. Entering a recovery period with high IMAT significantly compromises the cellular environment for healing, as demonstrated by Norris and colleagues (2025).
Frequently Asked Questions
Q1: Is intramuscular fat the same as being "skinny fat"? Related but distinct. "Skinny fat" (sometimes called TOFI — thin outside, fat inside) describes people with normal BMI but excess visceral fat and poor metabolic markers. Intramuscular fat can be elevated in TOFI individuals, but also in those who are visibly overweight. You do not need to look thin to have high IMAT — and you do not need to look heavy to have it, either. Joseph and colleagues (2025) confirm that BMI predicts IMAT imperfectly, highlighting the need for direct muscle quality assessment.
Q2: Can I tell if I have too much intramuscular fat without an MRI? Not with precision. However, functional warning signs include a noticeable loss of "spring" or push-off power when walking, difficulty rising from a low chair without using your arms, and reduced single-leg balance time. These reflect impaired ankle plantar flexor function — one of the earliest and most functionally consequential sites of fat infiltration, per Zhao and colleagues (2025). A physiotherapist can assess these markers without any imaging.
Q3: Does losing weight reduce muscle fat? Weight loss helps, but is not sufficient on its own. Caloric restriction without exercise tends to reduce subcutaneous fat while leaving intramuscular fat relatively unchanged — or even increasing it if lean muscle is lost alongside fat tissue. Exercise — particularly the combination of aerobic and resistance training — appears necessary to specifically target IMAT and improve IMCL metabolism (Razi et al., 2025). The vascular environment supporting muscle fat also needs rehabilitation, a process that exercise promotes through improved blood flow and anti-inflammatory signalling (AlZaim et al., 2026).
Q4: Are some people more genetically prone to intramuscular fat accumulation? Yes. Sex, age, and genetic factors all influence fat distribution patterns. Joseph and colleagues (2025) identified meaningful sex-based differences in where and how IMAT accumulates, with women and men showing distinct spatial patterns in thigh muscles. Hormonal changes with aging — declining oestrogen in women and testosterone in men — also alter fat partitioning toward muscle infiltration. Genetics influence baseline mitochondrial capacity, inflammatory tone, and FAP sensitivity, all of which modulate individual risk.
Q5: How does intramuscular fat relate to joint pain and arthritis? Increasingly, researchers recognise osteoarthritis as a whole-limb problem, not just a joint problem. IMAT in the thigh muscles — particularly the quadriceps that stabilise the knee — reduces force production, alters gait mechanics, and changes the loading patterns on cartilage. Joseph and colleagues (2025) used an osteoarthritis cohort specifically because IMAT is now considered a meaningful contributor to disease progression, not merely an incidental co-finding. Better muscle composition may be part of effective arthritis management.
Q6: Is it dangerous to exercise if I already have high intramuscular fat? The opposite is true — exercise is the most powerful tool for addressing it. The concern from the research is not that exercise is harmful in the presence of IMAT, but that standard rehabilitation may be less effective than expected if IMAT is very high, because the tissue environment is less conducive to repair (Norris et al., 2025). This argues for beginning an exercise programme before any planned procedure or immobilisation, not for avoiding exercise. Starting gently with Zone 2 aerobic work and progressing gradually is appropriate for most individuals.
Q7: What is the most exciting future treatment direction for reducing muscle fat? Several pharmacological targets are now under active investigation, including ceramide synthase inhibitors (which would block production of one of the most toxic lipid intermediates), mitochondrial-targeted antioxidants, and agents that modulate FAP differentiation directly. The dual roles of adipose tissue in muscle regeneration highlighted by Lu and colleagues (2026) suggest that any future drug will need to be carefully timed — preserving the early pro-regenerative functions of adipose signalling while blocking the chronic maladaptive ones. In the near term, exercise remains the most comprehensively effective intervention because it simultaneously addresses lipid oversupply, inflammation, and mitochondrial dysfunction (Razi et al., 2025).
Clinical pearls
1. Muscle Quality Over Muscle Quantity
Scientific Perspective: Sarcopenia and metabolic dysfunction are driven more by muscle quality (fat infiltration) than by absolute lean mass volume. High IMAT acts as a "stealth" driver of insulin resistance, even in individuals with normal BMIs.
Think of your muscle like a car engine. It doesn’t matter how big the engine is if the fuel lines are clogged with gunk. You can have large muscles, but if they are "marbled" with fat like a steak, they won't perform well or burn energy efficiently.
2. The FAP "Switch" and Tissue Reprogramming
Scientific Perspective: Fibro-adipogenic progenitors (FAPs) are the gatekeepers of muscle health. Chronic inflammation or inactivity flips their "switch" from supporting muscle repair to producing fat cells (adipogenesis).
Your body has specialised "repair cells" that can either fix muscle or turn into fat. When you are inactive or have high inflammation, these cells get the wrong instructions and start building fat inside the muscle instead of repairing the fibers.
3. The "Pre-hab" Imperative for Recovery
Scientific Perspective: Research by Norris et al. (2025) demonstrates that elevated IMAT creates a "hostile environment" that actively suppresses satellite cell activation and impairs force recovery after injury or surgery.
If you are planning for a surgery (like a knee replacement), "cleaning up" your muscle fat beforehand is vital. High muscle fat makes it harder for your body to heal afterward, regardless of how good your physical therapy is.
4. Vascular Architecture as a Limiting Factor
Scientific Perspective: The 2026 AlZaim study reveals that metabolic disease alters the vascular niche (blood vessel network) surrounding fat depots. This makes intramuscular fat resistant to mobilization and clearance through traditional weight loss alone.
ntramuscular fat isn't just "stored energy"; it builds its own plumbing system that keeps it locked in place. To get rid of it, you can't just eat less; you have to move to improve blood flow and "renovate" the environment inside the muscle.
5. Spatial Clustering and Fall Risk
Scientific Perspective: Fat doesn't accumulate evenly. In older adults, it clusters in specific compartments like the ankle plantar flexors, which are critical for balance correction and "push-off" power during walking.
You might lose your balance not because you are weak, but because fat is gathering in specific spots in your calves. This "fat clustering" acts like a glitch in your balance system, making it harder to catch yourself if you stumble.
6. The Athlete’s Paradox and Metabolic Flexibility
Scientific Perspective: Intramyocellular lipids (IMCL) are not inherently toxic; the danger lies in the accumulation of intermediates like ceramides and DAGs due to poor mitochondrial oxidation.
Having fat in your muscle is okay if you actually use it. Athletes have lots of muscle fat, but they burn it like high-quality fuel. In sedentary people, that same fat just sits there, goes "rancid," and blocks your body’s ability to handle sugar. The goal isn't to be fat-free; it's to be a "fat-burner."
Call to Action: Take the First Step Toward Muscle Quality
Ready to move from awareness to action? Start with these steps this week:
Day 1–3: Add a 10-minute walk after your two largest meals. No equipment needed.
Day 4: Try slow squats — lower yourself into a chair over 4 full seconds, stand normally. Repeat 10 times. Feel the difference in your legs.
Daily: Swap one snack for a handful of berries or a cup of green tea.
This month: Ask your GP or physiotherapist to assess your functional muscle quality — single-leg balance, timed sit-to-stand — not just your weight.
Author’s Note
As an Internal Medicine physician, I have increasingly come to view metabolic health through the lens of muscle quality, not simply body weight or muscle size. In clinical practice, I often see patients who appear outwardly “healthy” by conventional measurements yet struggle with fatigue, insulin resistance, declining mobility, slow recovery after illness, or unexplained loss of physical resilience. Modern research now helps explain why: the biology inside skeletal muscle matters profoundly.
One of the most important shifts in contemporary metabolic science is the recognition that skeletal muscle is not merely a structure for movement — it is one of the body’s most powerful metabolic organs. Healthy muscle regulates glucose disposal, mitochondrial energy production, inflammation control, physical stability, and healthy aging. But when fat begins infiltrating muscle tissue, these functions gradually become compromised long before obvious disease develops.
What makes intramuscular fat especially important is that it often develops silently. Many individuals with high levels of intramuscular adipose tissue (IMAT) or intramyocellular lipid accumulation (IMCL) may still appear physically normal, maintain a stable body weight, or even remain moderately active. Yet beneath the surface, metabolic flexibility, insulin sensitivity, and regenerative capacity may already be deteriorating.
The encouraging message is that this process is highly modifiable. Exercise, sleep quality, nutrition, stress reduction, and consistent physical activity remain extraordinarily powerful interventions because they target the root biological pathways driving muscle dysfunction — inflammation, mitochondrial impairment, oxidative stress, and impaired lipid metabolism.
My goal with this article is not to create fear around aging or body composition, but to help readers understand that improving muscle health is about far more than aesthetics. Preserving strong, metabolically healthy muscle may be one of the most important investments we can make for long-term mobility, independence, cardiovascular health, and healthy aging
References
AlZaim, I., Hassan, M. N., Schröter, M., et al. (2026). Defining the vascular niche of human adipose tissue across metabolic states. Nature Metabolism, 8, 722–740. https://doi.org/10.1038/s42255-026-01475-2
Jones, H. G., Kopinke, D., & Meyer, G. A. (2025). Intramuscular adipose tissue: From progenitor to pathology. American Journal of Physiology–Cell Physiology, 329(4), C1268–C1282. https://doi.org/10.1152/ajpcell.00613.2025
Joseph, G. B., Akkaya, Z., Sims, W. M., et al. (2025). MRI-based analysis of thigh intramuscular fat and its associations with age, sex, and BMI using data from the osteoarthritis initiative data. Scientific Reports, 15, 6188. https://doi.org/10.1038/s41598-024-75005-z
Lu, C., Lu, F., & Cai, J. (2026). Dual roles of adipose tissue in skeletal muscle regeneration: Pro-regenerative versus maladaptive. Journal of Cachexia, Sarcopenia and Muscle. Advance online publication. https://doi.org/10.1002/jcsm.70269
Norris, A. M., Palzkill, V. R., Appu, A. B., Fierman, K. E., Noble, C. D., Ryan, T. E., & Kopinke, D. (2025). Intramuscular adipose tissue restricts functional muscle recovery. Cell Reports, 44(8), 116021. https://doi.org/10.1016/j.celrep.2025.116021
Razi, O., De Moraes, C., Zamani, N., Saeidi, A., Hadjicharalambous, M., Hackney, A. C., Del Coso, J., Laher, I., & Zouhal, H. (2025). From obesity to muscle insulin resistance: The mediating roles of intramyocellular lipids, inflammation, and oxidative stress. Diabetes/Metabolism Research and Reviews, 41(7), e70094. https://doi.org/10.1002/dmrr.70094
Zhao, Z., Smith, F. E., Dick, T. J. M., & Hodson-Tole, E. (2025). Age-related differences in intramuscular fat distribution: Spatial quantification in human ankle plantar flexors. Frontiers in Bioengineering and Biotechnology, 13, 1594557. https://doi.org/10.3389/fbioe.2025.1594557