PCOS Is Being Renamed in 2026: What the New Science Means for Women
Doctors say the term “PCOS” no longer reflects the true biology of the condition. Learn why PMOS may replace PCOS and what it means for treatment and diagnosis.
METABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/15/202613 min read
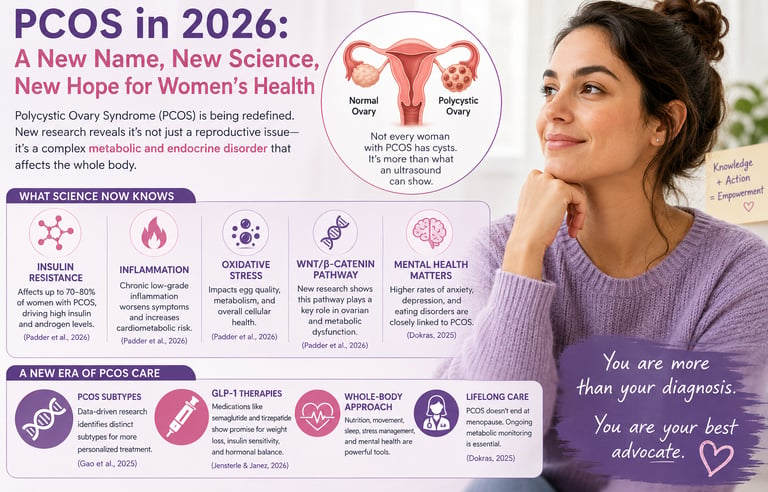
For decades, millions of women diagnosed with polycystic ovary syndrome (PCOS) were told they simply had a “hormonal imbalance” — a vague explanation that rarely captured the full complexity of what was happening inside their bodies. But in 2026, that understanding is changing dramatically. Researchers now recognize that PCOS is far more than irregular periods or ovarian cysts. It is increasingly viewed as a complex metabolic and endocrine disorder involving insulin resistance, chronic inflammation, altered hormone signaling, gut-metabolic interactions, and elevated long-term cardiometabolic risk (Teede et al., 2026).
This shift in understanding is so significant that global experts have proposed renaming the condition Polyendocrine Metabolic Ovarian Syndrome (PMOS) to better reflect its systemic nature and lifelong health implications (Teede et al., 2026). At the same time, breakthrough studies are revealing that PCOS may not be a single condition at all, but rather a spectrum of biologically distinct PCOS subtypes, each with unique metabolic and reproductive features (Gao et al., 2025).
The implications are enormous. Scientists are now exploring precision medicine approaches, personalized nutrition strategies, and advanced therapies, including GLP-1 receptor agonists such as semaglutide and tirzepatide for women struggling with insulin resistance, PCOS, obesity, infertility, and metabolic dysfunction (Jensterle & Janez, 2026).
For patients, this new wave of research offers something many have waited years to hear: clearer answers, more individualized treatment pathways, and renewed hope that PCOS care is finally catching up with the science.
What Is PCOS? A Quick Primer
Polycystic ovary syndrome is a complex hormonal disorder characterized by a trio of features: irregular or absent menstrual cycles, elevated levels of androgens (male hormones like testosterone), and the appearance of multiple small cysts on the ovaries on ultrasound. Not every woman with PCOS has all three, which is part of what makes diagnosis so tricky.
Beyond reproductive health, PCOS is deeply intertwined with metabolic dysfunction — insulin resistance, type 2 diabetes risk, cardiovascular disease, obesity, anxiety, and depression are all associated conditions. This is not just a "period problem." It is a whole-body syndrome with lifelong health implications.
And yet, for too long, the medical community has treated it as though it were one-size-fits-all. New research is rapidly dismantling that assumption.
Women with PCOS have a ~4-fold increased risk of type 2 diabetes.
Up to 70% of women remain undiagnosed.
Weight loss of 5–10% may restore ovulation.
Breaking News: PCOS Is Being Renamed
In a landmark Health Policy paper published in The Lancet (May 12, 2026), an international team led by Prof. Helena J. Teede and colleagues announced the renaming of Polycystic Ovary Syndrome (PCOS) to Polyendocrine Metabolic Ovarian Syndrome (PMOS).Teede et al. (2026).
Why Experts Want to Rename PCOS
The name is misleading: Many women diagnosed with PCOS do not actually have polycystic ovaries on ultrasound. The term focuses on a feature that is neither universal nor required for diagnosis.
It ignores the metabolic roots of the condition: PCOS is far more than an ovarian disorder. It involves major metabolic and endocrine abnormalities including insulin resistance, androgen excess, chronic inflammation, and dysfunction across multiple hormonal systems.
The current term minimizes disease complexity: The proposed name — Polyendocrine Metabolic Ovarian Syndrome (PMOS) — better reflects the condition’s whole-body impact on metabolism, hormones, fertility, cardiovascular health, and long-term disease risk.
The word “cysts” creates unnecessary fear and stigma: Many patients report confusion, shame, anxiety, and body-image distress after hearing the diagnosis, even though the “cysts” are actually immature follicles, not dangerous ovarian cysts.
A new name may improve awareness and treatment: Experts believe more scientifically accurate terminology could help clinicians recognize PCOS earlier, encourage comprehensive metabolic screening, and reduce years of underdiagnosis and misunderstanding.
PCOS Is Not One Condition — It's Several: The Subtype Revolution
Perhaps the most exciting scientific development of 2025 is the identification of distinct, data-driven subtypes of PCOS, published in the prestigious journal Nature Medicine.
Gao, Zhao, Du, and colleagues (2025) applied advanced machine-learning algorithms to large-scale clinical datasets, allowing the data itself to reveal patterns rather than relying on researcher assumptions. The result? Multiple biologically distinct subtypes of PCOS, each with different hormonal profiles, metabolic features, and clinical outcomes — including different risks for diabetes, cardiovascular disease, and infertility.
Why This Matters for You
For years, two women could both be diagnosed with PCOS and given essentially the same treatment, despite having very different underlying biology. One might have predominantly metabolic dysfunction with insulin resistance driving most of her symptoms; another might have a primarily reproductive subtype with fewer metabolic complications. One might respond well to metformin; another might not.
The findings from Gao et al. (2025) suggest that the era of personalized PCOS treatment is finally within reach. In the near future, your doctor may be able to identify your specific PCOS subtype and tailor your treatment plan accordingly — choosing the right medications, lifestyle interventions, and fertility strategies for your biology, not a generic patient.
This research also helps explain a long-standing puzzle: why do women with PCOS have such wildly different experiences? The answer may simply be that "PCOS" is an umbrella term covering several distinct conditions that have been lumped together out of clinical necessity.
Insights and Innovations: The State of PCOS Care
Writing in Fertility and Sterility, Dokras (2025) provides a comprehensive overview of where PCOS science stands today — and the picture is both sobering and hopeful.
The sobering part: PCOS remains chronically underdiagnosed, often taking years and multiple healthcare visits before a woman receives an accurate diagnosis. Mental health dimensions — including significantly elevated rates of depression, anxiety, and eating disorders — are frequently overlooked in routine care. And health disparities mean that women of color, women in low-income settings, and women in countries without robust gynecological infrastructure are disproportionately underserved.
The hopeful part: Research investment in PCOS has accelerated dramatically. New diagnostic frameworks, biomarker discoveries, and treatment pipelines are advancing faster than at any previous point in history. Dokras (2025) highlights particularly promising developments in understanding PCOS across the lifespan — recognizing that the condition does not end at menopause and requires long-term management strategies that evolve with the patient's life stage.
The key message: PCOS is finally being taken seriously as the complex, lifelong condition it is.
The Molecular Puzzle: Why PCOS Affects So Much of Your Body
A comprehensive review published in Molecular Biology Reports by Padder, Ganie, Jahan, and colleagues (2026) sheds new light on the biological mechanisms that underlie the far-reaching effects of PCOS.
Insulin Resistance: The Central Driver
Insulin resistance — when cells stop responding normally to insulin — is present in up to 70–80% of women with PCOS, even those who are not overweight. When insulin stops working properly, the body compensates by producing more of it. These elevated insulin levels then stimulate the ovaries to produce excess androgens (male hormones), disrupting the hormonal balance necessary for regular ovulation.
This is why PCOS is so strongly associated with type 2 diabetes risk, and why managing blood sugar is central to PCOS treatment regardless of weight.
Inflammation: A Slow Burn
Padder et al. (2026) highlight that chronic low-grade inflammation is a hallmark of PCOS. Elevated levels of inflammatory markers — including C-reactive protein and various cytokines — are consistently found in women with the condition. This inflammation contributes to insulin resistance, worsens cardiovascular risk, and may directly impair ovarian function.
Dietary patterns, gut microbiome health, and stress levels all influence this inflammatory state, which is why lifestyle interventions are not merely "nice to have" but genuinely therapeutic.
Oxidative Stress: When Your Cells Are Under Attack
Oxidative stress — an imbalance between harmful free radicals and the body's antioxidant defences — is significantly elevated in PCOS, according to Padder et al. (2026). This cellular-level stress impairs oocyte (egg) quality, damages blood vessel walls, and amplifies insulin resistance. It may help explain why PCOS affects fertility even in women who appear to ovulate regularly.
The WNT/β-Catenin Pathway: A Newly Emerging Piece
Padder et al. (2026) provide a comprehensive review exploring the complex interplay between insulin resistance (IR), chronic low-grade inflammation (LGI), oxidative stress (OS), and dysregulated WNT/β-catenin signaling in the pathophysiology of Polycystic Ovary Syndrome (PCOS).
The authors highlight that PCOS is a multifactorial disorder where these mechanisms do not act in isolation but form a vicious cycle. Insulin resistance promotes hyperandrogenism and ovulatory dysfunction, while chronic inflammation and elevated oxidative stress further exacerbate insulin signaling defects and ovarian dysfunction. The review emphasizes the emerging role of dysregulated WNT/β-catenin pathway, which influences follicle development, steroidogenesis, and metabolic homeostasis.
Despite significant progress in understanding these interconnected pathways, the exact etiological mechanisms remain incompletely understood. The authors conclude that deeper insight into these molecular crosstalks is crucial for identifying reliable biomarkers and developing novel therapeutic targets for more effective PCOS management.
The GLP-1 Revolution: Can Weight-Loss Drugs Transform PCOS Care?
The headlines have been impossible to miss: GLP-1 receptor agonists — medications originally developed for diabetes and now famous for their dramatic weight-loss effects — are transforming metabolic medicine. Drugs like semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound) are being studied across virtually every metabolic condition known to medicine. PCOS is no exception.
A comprehensive evidence map published in Drugs by Jensterle and Janez (2026) reviews the accumulating data on incretin-based anti-obesity medications — including GLP-1 receptor agonists and GIP/GLP-1 dual agonists — specifically in women with PCOS.
What the Research Shows
The findings are genuinely exciting. In women with PCOS, these medications appear to:
Reduce body weight significantly, which in turn reduces androgen levels and restores menstrual regularity in many patients.
Improve insulin sensitivity, directly addressing one of the core mechanisms of PCOS.
Reduce inflammation and oxidative stress markers.
Improve ovulation rates, raising the possibility that these medications could support fertility — a question currently under active investigation.
Improve psychological well-being, including reductions in anxiety and depression symptoms, likely mediated by both weight loss and direct effects on brain chemistry.
Jensterle and Janez (2026) are careful to note that the evidence base is still maturing. Many studies are small and short-term, and long-term safety data specific to women with PCOS — especially those who may wish to conceive — are still being gathered. These are not yet standard first-line treatments, but they represent one of the most promising therapeutic frontiers in PCOS care.
Important Note: Never start or stop any medication without consulting your healthcare provider. This is particularly important for women who are pregnant, breastfeeding, or actively trying to conceive.
Practical Applications: What You Can Do Right Now
Science is moving fast, but you don't have to wait for future treatments to start supporting your health today. Based on the latest evidence, here are actionable steps grounded in current research:
1. Prioritize Blood Sugar Balance — Every Day
Since insulin resistance is central to most PCOS cases, managing blood sugar is foundational. Focus on:
Eating a low-glycemic-index diet rich in fiber, lean proteins, and healthy fats.
Avoiding refined carbohydrates and ultra-processed foods that spike blood sugar rapidly.
Never skipping meals, which can worsen insulin dysregulation.
Pairing carbohydrates with protein and fat at every meal to blunt glucose spikes.
2. Move Your Body in Ways That Improve Insulin Sensitivity
Both aerobic exercise and strength training improve insulin sensitivity. Aim for at least 150 minutes of moderate-intensity movement per week, incorporating resistance training at least twice weekly. Even short walks after meals measurably reduce post-meal blood sugar.
3. Address Inflammation Through Diet
An anti-inflammatory eating pattern — Mediterranean-style, rich in vegetables, fruits, legumes, whole grains, olive oil, and oily fish — directly targets the chronic inflammation identified as a PCOS driver by Padder et al. (2026). Minimize alcohol, processed meats, and refined sugars.
4. Protect Your Mental Health Proactively
The mental health burden of PCOS is real and significant. Seek evaluation and support for anxiety, depression, or disordered eating — these are medical issues, not personal failures. Cognitive behavioral therapy (CBT) has strong evidence in this population.
5. Ask Your Doctor About Your PCOS Subtype
As subtype research advances, ask your endocrinologist or gynecologist whether any specialized testing could help clarify your dominant PCOS profile — whether primarily metabolic, reproductive, or inflammatory. This conversation alone can shape a more personalized treatment plan.
6. Track Your Symptoms Systematically
Keep a detailed log of your menstrual cycles, energy levels, skin changes, mood, sleep quality, and weight. Apps like Clue, Flo, or Natural Cycles can help. This data is invaluable for your healthcare team and can accelerate diagnosis and treatment refinement.
7. Advocate for Comprehensive Screening
Ensure you are being screened for the full spectrum of PCOS-associated conditions: glucose tolerance, lipid profiles, blood pressure, thyroid function, and mental health. PCOS requires a multidisciplinary approach — reproductive endocrinology, nutrition, mental health, and primary care working together.
Frequently Asked Questions About PCOS in 2026
Q1: What is the new name for PCOS, and will my diagnosis change?
The proposed new name is Polyendocrine Metabolic Ovarian Syndrome (PMOS), recommended by a global consensus process led by Teede and colleagues (2026). If adopted, your underlying condition remains the same — only the label changes, to better reflect the metabolic and endocrine complexity of the syndrome. Speak with your doctor about how this may affect your records and care.
Q2: Can I have PCOS without polycystic ovaries on ultrasound?
Yes, absolutely. A diagnosis of PCOS does not require visible cysts on ultrasound. In fact, part of why the name change is being advocated is that the "polycystic" label is misleading — many women with PCOS don't have them, and the ovarian ultrasound finding alone is not diagnostic.
Q3: Are GLP-1 medications like Ozempic right for me if I have PCOS?
Possibly, but this is a decision to make with your doctor. Jensterle and Janez (2026) summarize promising evidence, including improvements in weight, hormonal profiles, and menstrual regularity. However, these medications are not yet standard first-line PCOS treatments, and data on long-term outcomes and safety in women trying to conceive are still emerging. Do not self-prescribe.
Q4: Does PCOS go away after menopause?
No. While some reproductive symptoms resolve with menopause, the underlying metabolic risks — including elevated cardiovascular disease, diabetes, and metabolic syndrome risk — persist throughout life. Women with PCOS require ongoing metabolic monitoring well beyond their reproductive years, as highlighted by Dokras (2025).
Q5: Is PCOS genetic? Will my daughter inherit it?
PCOS has a significant heritable component, though it is not caused by a single gene. If you have PCOS, your daughters and sisters have a higher risk. This makes early awareness and screening especially important for families with a history of the condition.
Q6: Can women with PCOS get pregnant naturally?
Many can, yes. PCOS is the most common cause of ovulatory infertility, but it is often treatable. Weight management, lifestyle modification, and medications like letrozole or clomiphene can successfully induce ovulation in many women. Advances in understanding PCOS subtypes (Gao et al., 2025) may further refine fertility treatment selection in coming years.
Q7: What does insulin resistance have to do with my acne and hair loss?
Everything, potentially. When insulin is elevated due to insulin resistance, it stimulates the ovaries and adrenal glands to produce excess androgens (male hormones like testosterone). These androgens drive many of the most visible PCOS symptoms: acne along the jawline, excess facial or body hair (hirsutism), scalp hair thinning, and oily skin. Treating insulin resistance — through diet, exercise, or medication — can meaningfully improve these symptoms.
Clinical pearls.
1. The Name Change: From "Cysts" to "Systems"
Scientific Insight: The proposed rename to PMOS reflects that the condition is a systemic endocrine and metabolic disorder rather than a localized ovarian issue. Polycystic ovaries are a symptom, not the cause, and are absent in many clinical presentations.
Don't let the word "polycystic" confuse you. You can have PCOS without a single cyst on your ovaries. The new name, PMOS, highlights that this is a whole-body hormonal and metabolic journey, not just a "period problem."
2. The Insulin-Androgen Feedback Loop
Scientific Insight: Hyperinsulinemia (excess insulin) acts as a co-gonadotropin, directly stimulating the ovarian theca cells to produce excess androgens. This makes insulin resistance a primary driver of hirsutism and acne, regardless of body mass index (BMI).
Think of insulin as a "volume knob" for your male hormones. When your insulin levels are high, they tell your ovaries to crank up the testosterone. Managing your blood sugar isn't just about weight—it’s often the secret to clearing your skin and slowing unwanted hair growth.
3. Precision Medicine: Identifying Your Subtype
Scientific Insight: Machine-learning advances (Gao et al., 2025) have identified distinct subtypes—such as Metabolic vs. Reproductive dominant profiles. These subtypes dictate different risks for Type 2 Diabetes and different responses to treatments like Metformin or Letrozole.
PCOS isn't "one size fits all." You and a friend might both have PCOS but require completely different treatments. Ask your doctor about your specific profile: is your struggle mainly metabolic (blood sugar), reproductive (ovulation), or inflammatory? Knowing your "type" helps you target your treatment.
4. Chronic Low-Grade Inflammation
Scientific Insight: PCOS is characterized by elevated pro-inflammatory cytokines and oxidative stress markers. This chronic inflammation worsens insulin resistance and can impair oocyte (egg) quality even when ovulation is achieved.
PCOS involves a "slow burn" of inflammation in the body. This is why lifestyle isn't just about calories; it’s about cooling that fire. Anti-inflammatory foods like leafy greens, berries, and fatty fish act like a natural "buffer" for your cells and your fertility.
5. The "Incretin Revolution" (GLP-1s)
Scientific Insight: New data on GLP-1 and GIP/GLP-1 receptor agonists (like tirzepatide) show they address the core pathophysiology of PCOS by improving insulin signaling and reducing visceral adiposity, which can restore the hypothalamic-pituitary-ovarian axis.
Newer metabolic medications (like those used for weight loss) are showing huge promise for PCOS. They don't just help with weight; they help reset how your body processes sugar and hormones. If traditional treatments haven't worked, it’s worth asking your specialist about these "incretin" options.
6. A Lifelong Metabolic Horizon
Scientific Insight: The health risks of PCOS (PMOS) do not terminate at menopause. While reproductive symptoms may ease, the risk for cardiovascular disease, non-alcoholic fatty liver disease (NAFLD), and metabolic syndrome remains elevated throughout the post-menopausal years.
Your PCOS journey doesn't end when your periods do. Because it affects your metabolism, you need to keep an eye on your heart health and blood sugar even after menopause. Think of your PCOS diagnosis as a lifelong "health dashboard" that helps you prevent issues before they start.
Author’s Note
As clinicians, we are witnessing a major turning point in how the medical community understands and manages polycystic ovary syndrome (PCOS). For many years, PCOS was viewed primarily as a reproductive disorder centered around irregular periods, infertility, and ovarian cysts. However, emerging evidence now makes it clear that this condition extends far beyond gynecology. PCOS is increasingly recognized as a complex metabolic and endocrine syndrome involving insulin resistance, chronic inflammation, altered androgen signaling, and elevated long-term cardiometabolic risk.
In everyday clinical practice, we continue to see women who spend years searching for answers before receiving an accurate diagnosis. Many struggle not only with physical symptoms such as weight gain, acne, hirsutism, and fertility challenges, but also with anxiety, depression, body-image distress, and frustration from feeling misunderstood within healthcare systems. This gap between patient experience and traditional medical understanding is precisely why the evolving science surrounding PCOS is so important.
The proposed shift toward the term Polyendocrine Metabolic Ovarian Syndrome (PMOS) reflects more than a name change — it represents a broader clinical recognition that PCOS is a whole-body disorder requiring multidisciplinary, long-term care. Advances in subtype research, metabolic medicine, lifestyle therapeutics, and incretin-based therapies are opening the door to more personalized and biologically targeted treatment approaches.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
The BMI Paradox: Why "Normal Weight" People Still Get High Blood Pressure | DR T S DIDWAL
How Insulin Resistance Accelerates Cardiovascular Aging | DR T S DIDWAL
The Metabolic Triad: Why Diabetes, Obesity & CVD Are One Epidemic | DR T S DIDWAL
References
Dokras, A. (2025). Polycystic ovary syndrome in 2025—insights and innovations. Fertility and Sterility. Advance online publication. https://doi.org/10.1016/j.fertnstert.2025.09.025
Gao, X., Zhao, S., Du, Y., et al. (2025). Data-driven subtypes of polycystic ovary syndrome and their association with clinical outcomes. Nature Medicine, 31, 4214–4224. https://doi.org/10.1038/s41591-025-03984-1
Jensterle, M., & Janez, A. (2026). Incretin-based anti-obesity medications in polycystic ovary syndrome: The evidence map. Drugs. https://doi.org/10.1007/s40265-026-02325-x
Padder, K. A., Ganie, M. A., Jahan, N., et al. (2026). Insulin resistance, inflammation, oxidative stress and dysregulated WNT/β-Catenin signaling in polycystic ovary syndrome: A review. Molecular Biology Reports, 53, 703. https://doi.org/10.1007/s11033-026-11889-6
Teede, H. J., Khomami, M. B., Morman, R., Laven, J. S. E., Joham, A. E., Costello, M. F., Patil, M., Rees, D. A., Berry, L., Cree, M. G., Zhao, H., Norman, R. J., Dokras, A., & Piltonen, T. (2026). Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome: A multistep global consensus process. The Lancet. Advance online publication. https://doi.org/10.1016/S0140-6736(26)00717-8