Can Muscle Loss Be Reversed? Scientists Discover the FoxO–DEAF1–mTOR Pathway Behind Muscle Aging
Can muscle loss be prevented? Discover how FoxO, DEAF1, NF-κB and mTOR control muscle growth, autophagy and sarcopenia using the latest evidence.
SARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/10/202621 min read
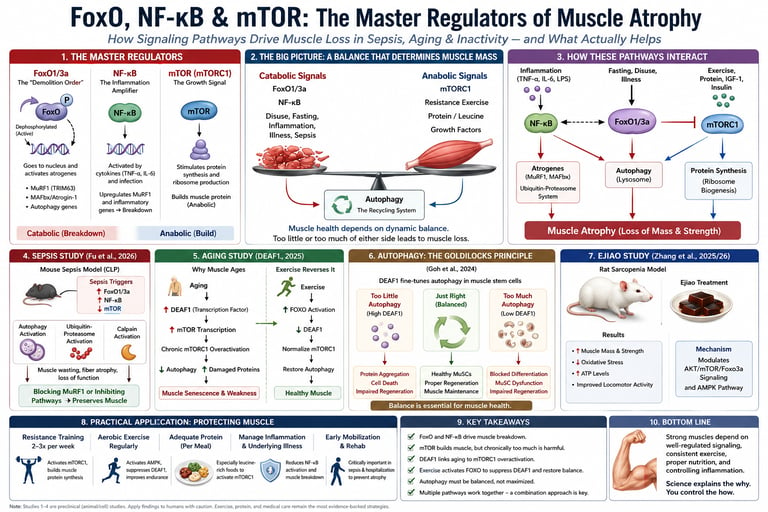
Muscle atrophy occurs when muscle protein breakdown exceeds protein synthesis. The key molecular regulators are FoxO1/3a, NF-κB, mTOR, and autophagy. During aging, sepsis, or inactivity, FoxO and NF-κB activate protein degradation pathways, while disrupted mTOR signaling impairs muscle repair. Regular resistance exercise, adequate protein intake, and early rehabilitation remain the most effective evidence-based strategies to preserve muscle mass and strength.
KEt takeaways
1. Muscle Loss is an Active Dynamic, Not Just "Fading Away"
Muscle atrophy is not just a passive consequence of sitting still or getting older. It is an actively regulated cellular process. It occurs when your body's internal signaling systems tilt the scales, causing protein degradation (breakdown) to move faster than protein synthesis (building).
2. FoxO1 and FoxO3a: The Dual-Nature Demolition Switches
FoxO1 and FoxO3a are transcription factors—proteins that act like light switches for specific genes. During periods of starvation, severe illness, or prolonged bed rest, they enter the cell nucleus and turn on "atrogenes" (genes that command the cell to dismantle its own structure). However, they aren't purely villainous; during exercise, FoxO activation is actually required to help reset and protect aging muscle.
3. NF-κB: The Inflammation Amplifier in Acute Illness
When the body faces a massive inflammatory storm—such as during sepsis or critical illness—a signaling switch called NF-κB fires up. It acts as an amplifier for inflammation, working side-by-side with FoxO to rapidly accelerate muscle breakdown. This explains why patients in the ICU can lose a visible amount of muscle mass in just a few days.
4. The mTOR Paradox: More is Not Always Better
mTOR (specifically mTORC1) is the body’s primary "growth engine" that triggers muscle building in response to protein intake and resistance training. While too little mTOR activity causes muscle to waste away, chronically overactive mTOR is equally damaging. It creates a traffic jam inside the cell, preventing old, broken proteins from being cleared out.
5. The DEAF1 Discovery: Why Aging Muscle Struggles
A groundbreaking 2025 study identified a genetic accelerator pedal called DEAF1 that rises naturally as we age. DEAF1 keeps the mTOR growth engine constantly revved up in old muscle. Instead of making the muscle bigger, this constant overactivation causes cellular exhaustion and stops the muscle from repairing itself properly.
6. Exercise is a Molecular Reset Button
The most exciting takeaway from recent aging research is that structured exercise directly counteracts the DEAF1 aging pathway. When you move, FoxO is activated in a healthy way, which steps in to suppress DEAF1. This brings the overactive mTOR engine back down to a normal, healthy operating speed, clearing out cellular clutter and restoring muscle vitality.
7. Autophagy Requires a "Goldilocks" Balance
Autophagy is your cells' internal recycling system, responsible for eating up damaged components. Popular health trends often emphasize maximizing autophagy through extreme fasting. However, muscle stem cell science shows that muscle health requires a perfect middle ground. Too much or too little autophagy disrupts your muscle's ability to heal and regenerate after an injury.
8. Preclinical Leads vs. Real-World Solutions
While traditional remedies like Ejiao (donkey-hide gelatin) and experimental pharmaceutical compounds show fascinating promise in regulating these identical pathways (AKT/mTOR/FoxO) in rodent models, they are still "preclinical." Today, the most reliable, human-proven ways to protect your muscle through illness, injury, and aging remain early mobilization, progressive resistance training, and properly timed dietary protein.
If you've ever watched a hospitalized loved one lose visible muscle in a matter of days, or noticed your own strength quietly slipping away in your 50s and 60s, you've witnessed the same underlying biology at work: skeletal muscle atrophy.
Muscle wasting isn't one disease. It's the output of a small set of molecular switches that your body uses in very different situations — critical illness, disuse, cancer, and normal aging — to decide whether muscle tissue gets built up or broken down. Three of those switches come up again and again in the newest research: FoxO1/FoxO3a, NF-κB, and mTOR.
1. What Is Muscle Atrophy?
Muscle atrophy is the loss of muscle fiber size and mass. It happens whenever the rate of muscle protein breakdown outpaces the rate of muscle protein synthesis. That balance is controlled almost entirely by signaling pathways inside muscle cells — not simply by how much you eat or how little you move, though both matter enormously.
Clinically, muscle atrophy shows up in very different settings:
Critical illness and sepsis — rapid, severe muscle loss within days of ICU admission, associated with longer ventilator time and worse survival.
Sarcopenia — the slow, progressive loss of muscle mass and strength with normal aging, affecting an estimated 10–27% of older adults depending on the diagnostic criteria used.
Disuse atrophy — from bed rest, limb immobilization, or a sedentary lifestyle.
Cachexia — muscle wasting driven by cancer, heart failure, or chronic kidney disease.
Despite looking different on the outside, these conditions converge on the same handful of intracellular signaling pathways. That convergence is exactly why FoxO, NF-κB, mTOR, and autophagy have become the central focus of muscle-wasting research over the last two decades — and why targeting them is now considered one of the most promising strategies for future treatments.
2. Meet the Master Regulators: FoxO1/3a, NF-κB, and mTOR
Think of a muscle fiber as a small factory. It has to decide, moment to moment, whether to build new proteins (machinery, structure) or break old ones down for recycling and energy. Three regulators make that call.
FoxO1 and FoxO3a: The "Demolition Order" Transcription Factors
FoxO1 and FoxO3a are transcription factors — proteins that switch genes on and off. When they're active, they turn on genes for two of the body's main protein-degradation systems:
The ubiquitin-proteasome system, via genes like MuRF1 (also called Trim63) and MAFbx/atrogin-1, often collectively called "atrogenes."
Autophagy-related genes, which trigger the cell to digest its own components.
Under normal conditions, growth signals like insulin and IGF-1 keep FoxO proteins phosphorylated and inactive, tucked outside the nucleus. Illness, fasting, disuse, and inflammation all reverse that — FoxO moves into the nucleus and starts issuing demolition orders.
NF-κB: The Inflammation Amplifier
NF-κB is the master switch for inflammatory gene expression. In muscle, chronic NF-κB activation — driven by inflammatory cytokines like TNF-α and IL-6, which surge during infection and sepsis — directly increases expression of MuRF1 and promotes muscle protein breakdown. Notably, research has shown that blocking both NF-κB and FoxO activity simultaneously can nearly eliminate disuse-induced muscle fiber atrophy in animal models, because many atrophy genes have binding sites for both regulators sitting side by side in their promoter regions.
mTOR: The Growth Signal
mTOR (mechanistic target of rapamycin), particularly as part of the mTORC1 complex, is the primary driver of muscle protein synthesis. When mTORC1 is active, it tells the cell to build new muscle protein and ramp up ribosome production. Resistance exercise and adequate dietary protein (especially leucine) are the two most reliable ways to activate mTORC1 in humans.
Here's the twist that surprises a lot of people: too little mTOR activity causes atrophy, but chronically too much mTOR activity can also be harmful. As you'll see in the aging section below, sustained mTORC1 overactivation in old muscle disrupts the cell's ability to clear damaged proteins, contributing to sarcopenia rather than preventing it. Muscle health depends on this pathway being appropriately dynamic — ramping up after a workout, then coming back down — not simply "high" or "low."
How the Three Interact
Regulator Primary Role Activated By Net Effect on Muscle FoxO1/3a Turns on protein-degradation genes Fasting, illness, disuse, low insulin/IGF-1 signaling Breakdown (catabolic) NF-κB Drives inflammatory gene expression Cytokines (TNF-α, IL-6), infection, sepsis Breakdown (catabolic) mTOR (mTORC1) Drives protein synthesis Resistance exercise, dietary protein/leucine, growth factors Growth (anabolic), but chronically excessive activity impairs autophagy
3. Sepsis and Muscle Wasting: Inside the 2026 Fu et al. Study
Sepsis — a life-threatening, dysregulated immune response to infection — is one of the fastest and most severe causes of muscle loss known in medicine. ICU patients can lose a measurable percentage of muscle cross-sectional area within the first week of critical illness, and that loss is strongly linked to prolonged mechanical ventilation, delayed rehabilitation, and higher mortality.
A 2026 study published in Scientific Reports by Fu and colleagues at Chongqing Medical University set out to map exactly which signaling pathways drive this process. Using a mouse model of sepsis (cecal ligation and puncture, a standard research method for inducing sepsis) alongside LPS-treated muscle cells in culture, the researchers found that <cite index="11-1">sepsis activates autophagy, the ubiquitin-proteasome system, and calpain pathways, resulting in muscle wasting and functional decline</cite>.
Key Mechanistic Findings
The study's central discovery was that these degradation systems don't switch on randomly — they're coordinated by upstream signaling changes. Specifically, the researchers found that <cite index="11-1">these changes were linked to upregulated FoxO1/3a and NF-κB signaling and suppressed mTOR activity</cite>. In other words, sepsis simultaneously flips on both "demolition" switches (FoxO and NF-κB) while shutting off the "build" switch (mTOR) — a coordinated catabolic assault on muscle tissue from three directions at once.
Perhaps most clinically relevant, when the researchers intervened — either with drugs that inhibit specific components, or by genetically deleting them, particularly MuRF1 — they found this <cite index="11-1">mitigated muscle atrophy and preserved function</cite> in the animal model.
Why This Matters (Clinical Interpretation)
This study doesn't hand doctors a new drug to prescribe tomorrow. What it does is sharpen the therapeutic target. Prior sepsis research (including a related 2026 study on STAT3 inhibition) has shown that different upstream pathways can converge on the same degradation machinery — but that blocking one pathway (like STAT3) may leave others, such as FoxO and NF-κB-driven autophagy, untouched. Researchers investigating STAT3 inhibition noted that autophagy in skeletal muscle is also regulated by <cite index="4-1">Foxo1/Foxo3 and the TLR4/NF-κB signaling cascade</cite>, which likely explains why single-pathway drugs haven't fully solved sepsis-related muscle wasting.
The practical implication for future treatment design is that combination approaches — targeting the ubiquitin-proteasome system (MuRF1 specifically) alongside upstream FoxO/NF-κB signaling — may be more effective than any single-pathway drug alone. This is exploratory, preclinical science; there is currently no approved medication that specifically targets FoxO1/3a-NF-κB-mTOR crosstalk in human sepsis patients. Muscle preservation during real-world sepsis treatment today still relies on early mobilization, adequate protein and calorie delivery, glycemic control, and physical therapy — the interventions with actual human trial support.
4. Why Muscle Ages: The DEAF1 Discovery (PNAS, 2025)
Sarcopenia — age-related muscle loss — has long been partly attributed to mTOR dysregulation, but the "why" behind that dysregulation was unclear until a landmark 2025 study from Duke-NUS Medical School.
The Paradox Researchers Had to Solve
mTORC1 is supposed to be a growth signal. So why does aging muscle, which is losing mass, show chronically overactive mTORC1? The Duke-NUS team, led by Hong-Wen Tang, explained the puzzle this way: <cite index="18-1">"The mTORC1 pathway is essential for muscle growth yet becomes chronically overactive in aging — a paradox that has made it challenging to pinpoint what drives this dysregulation."</cite>
Chronic mTORC1 overactivation in old muscle doesn't build more muscle — it actually impairs autophagy, the process that clears out misfolded and damaged proteins. Without that cleanup, damaged material accumulates inside muscle fibers, and function declines.
Discovering DEAF1 as the Upstream Driver
The researchers identified a transcription factor called DEAF1 as the missing link. Their findings showed that <cite index="15-1">elevated Deaf1 expression increases mTOR transcription, leading to heightened mTORC1 activity, impaired proteostasis, and muscle senescence</cite>. Put simply: DEAF1 is a gene-level accelerator pedal that gets pressed down harder as muscle ages, revving mTORC1 into a chronically overactive state.
The Exercise Reversal
Here's the part that has generated real excitement: the same team showed this process is reversible through exercise, not just theoretically blockable with a drug. In aged mice put through structured endurance exercise (including treadmill running), researchers observed that <cite index="15-1">exercise suppresses Deaf1 expression via FOXO activation, restoring mTORC1 balance and alleviating muscle aging</cite>.
This finding closes an elegant biological loop: FoxO transcription factors — the same "demolition order" regulators discussed above — aren't purely destructive. In this context, FoxO activation during exercise actively suppresses DEAF1, which in turn brings an overactive mTORC1 pathway back down to a healthy operating range. Context and dose determine whether FoxO activity helps or hurts.
The reversal isn't automatic, either. The researchers also found that <cite index="15-1">FOXO inhibition or Deaf1 overexpression blocks exercise benefits on muscle health</cite> — meaning the FOXO–DEAF1 axis is a required intermediate step, not just a correlated side effect. Follow-up commentary on the study noted that <cite index="16-1">exercise lowers DEAF1 levels, restores mTORC1 activity and autophagy gene expression, and improves autophagic flux without genetic manipulation, indicating that the autophagy defect is dynamically maintained</cite> — in other words, this age-related dysfunction is not a fixed, unchangeable feature of old muscle. It's an actively maintained state that a physiological stimulus (exercise) can shift back toward normal.
Clinical Interpretation
This is one of the more hopeful findings in recent sarcopenia research, because it identifies a specific molecular reason exercise is so effective against age-related muscle decline — beyond the generic explanation of "it builds more muscle." It also opens the door to future drugs that mimic exercise's effect on DEAF1 for patients who physically cannot exercise (due to frailty, injury, or severe illness). For now, though, the direct, human-validated lever remains the one the mice were given: structured physical activity, particularly a combination of aerobic and resistance training.
5. Autophagy: Your Muscle's Recycling System
Autophagy — literally "self-eating" — is the cellular process that clears out damaged proteins, dysfunctional mitochondria, and other cellular debris. It sounds like it should always be "bad" for muscle, since it involves breaking things down, but the opposite is often true: too little autophagy is just as harmful as too much.
A 2024 study in the journal Autophagy, from the same Duke-NUS research group that later published the DEAF1-exercise paper, laid the groundwork for understanding this balance at the level of muscle stem cells (MuSCs), which are essential for muscle repair after injury.
The researchers found that DEAF1 sits directly downstream of FOXO and functions as an autophagy brake: <cite index="26-1">Deaf1 is transcriptionally repressed by FOXOs and DEAF1 targets to Pik3c3 and Atg16l1 promoter regions and suppresses their expression</cite>. When DEAF1 is depleted, autophagy genes get switched back on — but that's not automatically good news either.
Critically, the study found a "Goldilocks" pattern: both too much and too little DEAF1 (and therefore both too much and too little autophagy) impaired muscle stem cell function. As the authors put it, <cite index="26-1">Deaf1 depletion therefore induces macroautophagy/autophagy, which in turn blocks MuSC survival and differentiation. In contrast, Deaf1 overexpression inactivates autophagy in MuSCs, leading to increased protein aggregation and cell death</cite>. Both extremes disrupted muscle regeneration — only a properly balanced, fine-tuned level of DEAF1/autophagy activity supported healthy repair.
This matters for the bigger picture: you cannot simply "maximize autophagy" and expect better muscle health. Popular wellness narratives sometimes treat autophagy as an unambiguous good to be pushed as high as possible (through prolonged fasting, for example). The actual biology of muscle stem cells says otherwise — autophagy needs to be regulated within a healthy range, not maximized. This is a case where nuance matters more than a slogan.
6. Traditional Medicine Meets Modern Signaling: The Ejiao Study
Not all muscle-signaling research comes from pharmaceutical labs — some of it is testing traditional remedies against the same modern molecular framework. A 2025/2026 study in the Journal of Ethnopharmacology examined Ejiao (donkey-hide gelatin, a traditional Chinese medicine ingredient historically used to "nourish blood and Qi") in a rat model of sarcopenia induced by D-galactose injections combined with restricted movement — a well-established way to simulate accelerated aging and disuse in animal research.
What the Researchers Found
Following Ejiao administration, the study reported that the treated rats showed <cite index="21-1">significant increases in body weight and gastrocnemius muscle mass, alongside improvements in locomotor activities, muscle morphology and pathology</cite>. The researchers also observed that Ejiao <cite index="21-1">effectively reduced oxidative stress in the sarcopenic rats, evidenced by decreased superoxide dismutase activity and tissue levels of the lipid peroxide malondialdehyde, while also enhancing ATP levels in the muscles</cite>.
Mechanistically, combined proteomic and metabolomic analysis pointed to the same signaling family covered throughout this article: the study concluded Ejiao's <cite index="21-1">benefits are mainly mediated through modulation of the AKT/mTOR/Foxo3a signaling pathway and the AMPK pathway, both crucial for protein synthesis and muscle function enhancement</cite>.
Clinical Interpretation and a Necessary Caveat
This is a genuinely interesting data point because it shows a traditional remedy converging on the exact same anabolic (AKT/mTOR) and catabolic (FoxO3a) signaling nodes that pharmaceutical researchers are targeting directly. It's consistent with a broader pattern in sarcopenia research: activating AMPK and normalizing AKT/mTOR/FoxO3a balance — through diet, exercise, or specific compounds — repeatedly shows up as protective against muscle loss in animal models.
That said, this was a rat study, not a human clinical trial, and Ejiao is a complex, multi-component substance whose donkey-hide-gelatin sourcing, dosing, and safety profile in aging or ill humans hasn't been established with the same rigor as, say, resistance training or protein supplementation. If you're considering Ejiao or any traditional remedy for muscle health, treat it as a supplement decision to discuss with your physician — particularly if you have any bleeding disorders, are on blood thinners, or have kidney or liver disease, since gelatin-based products can interact with these conditions.
7. How These Pathways Interact: The Big Picture
Pulling the four studies together, a consistent map emerges:
FoxO1/3a is the central switch that can turn on protein degradation (atrogenes, ubiquitin-proteasome system) or, in the specific context of exercise, suppress DEAF1 and help restore balanced mTOR signaling. Its effect depends entirely on the surrounding conditions and duration of activation.
NF-κB amplifies muscle breakdown almost exclusively in response to inflammation and infection, making it especially relevant in sepsis, critical illness, and chronic inflammatory conditions.
mTOR/mTORC1 needs to be dynamically regulated — insufficient during illness and starvation, appropriately activated after resistance exercise and protein intake, but harmfully chronic and unchecked in aging muscle when DEAF1 stays elevated.
Autophagy is the shared downstream process that both FoxO and mTOR ultimately influence, and it needs to stay in a healthy middle range — not suppressed, not maximized.
AMPK, the cell's energy sensor, generally works alongside FoxO3a to support healthy protein turnover and mitochondrial quality, and is activated by both exercise and (per the Ejiao data) certain nutritional compounds.
8. Practical Application: Protecting Muscle in Real Life
None of this research changes the fundamentals of muscle preservation — it explains why they work. Here's how to apply the science, organized by situation.
If You're Recovering From Illness, Surgery, or Hospitalization
Mobilize as early as safely possible. Even passive range-of-motion exercises and short walks, when cleared by your care team, counter the inflammatory (NF-κB) and catabolic (FoxO) drive toward muscle breakdown.
Prioritize protein intake during recovery. Illness and inflammation raise your protein needs; work with a registered dietitian or your medical team on a target, since needs vary by condition, kidney function, and severity of illness.
Ask about physical therapy and occupational therapy referrals — these remain the best human-trial-supported tools for limiting ICU-acquired and post-illness muscle loss.
If You're Focused on Preventing Age-Related Sarcopenia
Resistance train at least 2–3 times per week. This is the most direct, human-evidence-backed way to activate mTORC1 appropriately and, per the DEAF1 research, likely to help normalize the FoxO-DEAF1-mTOR axis over time.
Add aerobic/endurance activity. The DEAF1-reversal study specifically used endurance exercise (treadmill-style training) in aged mice — a reminder that "cardio" isn't just for your heart; it appears to matter for muscle-gene regulation too.
Eat adequate, well-distributed protein. Aim for protein at each meal (commonly cited ranges for older adults are higher than the general RDA — discuss a personalized target with a dietitian or physician, especially if you have kidney disease).
Don't chase "maximal autophagy." Based on the muscle stem cell research above, extreme or prolonged fasting practices aimed at maximizing autophagy are not clearly beneficial for muscle tissue specifically, and could theoretically disrupt the fine balance MuSCs need. Moderate, well-tolerated approaches are more defensible.
A Simple Weekly Framework
Here is your weekly schedule
Monday: Resistance Training
Focus: Target major muscle groups.
Why: Activates mTORC1 (a primary growth regulator) and directly stimulates muscle protein synthesis to build strength and mass.
Tuesday: Low-Intensity Cardio
Focus: Zone 2 cardio or a brisk walk.
Why: Supports AMPK activation (cellular energy sensing) and boosts overall cardiovascular health.
Wednesday: Mid-Week Break
Focus: Rest or light mobility work.
Why: Focuses on active recovery, allowing your body's anabolic (muscle-building) signaling pathways to consolidate.
Thursday: Resistance Training
Focus: Repeat stimulus for major muscle groups.
Why: Reinforces the muscle protein synthesis signaling triggered earlier in the week.
Friday: Higher-Intensity Cardio
Focus: Moderate-to-vigorous cardiovascular exercise.
Why: Mirrors the endurance-exercise stimulus shown to lower the aging-related protein DEAF1 in animal models.
Saturday: Flexible Training
Focus: Resistance training or active recovery.
Why: Highly adaptable depending on your current fatigue and recovery status.
Sunday: Rest Day
Focus: Full, passive recovery.
Why: Essential for tissue repair and long-term adaptation to your weekly training routine.
Always individualize this to your fitness level, medical conditions, and clearance from your healthcare provider — especially if you're recovering from illness, have cardiovascular disease, or are frail.
9. Evidence Summary Table
1. Sepsis-Induced Muscle Wasting (Fu et al., 2026, Scientific Reports)
Model: Mouse sepsis model (CLP) and LPS-treated C2C12 myotubes.
Key Pathways: FoxO1/3a ↑, NF-κB ↑, mTOR ↓.
Main Finding: Muscle wasting in sepsis is driven by the coordinated activation of three pathways: autophagy, ubiquitin-proteasome, and calpain. Targeting MuRF1 successfully mitigated muscle atrophy.
Evidence Level: Preclinical (animal/cell).
2. Aging and mTORC1 Overactivation (Choy, Goh, et al., 2025, PNAS)
Model: Aged mice subjected to endurance exercise.
Key Pathways: DEAF1 → mTORC1, FOXO.
Main Finding: The protein DEAF1 drives the chronic overactivation of mTORC1 in aged muscle. Endurance exercise helps suppress DEAF1 via FOXO, restoring a healthy metabolic balance.
Evidence Level: Preclinical (animal).
3. Muscle Stem Cell Regeneration (Goh et al., 2024, Autophagy)
Model: Drosophila (fruit flies), C2C12 cells, and primary mouse muscle stem cells (MuSCs).
Key Pathways: FOXO → DEAF1 → autophagy genes.
Main Finding: DEAF1 acts as a fine-tuner for autophagy. Both the loss and the overexpression of DEAF1 impair the regenerative capacity of muscle stem cells, indicating that precise balance is required.
Evidence Level: Preclinical (animal/cell).
4. Therapeutic Effects of Ejiao on Muscle Loss (Zhang et al., 2025/2026, J. Ethnopharmacology)
Model: D-galactose treated and restricted-movement rat model.
Key Pathways: AKT/mTOR/Foxo3a, AMPK.
Main Finding: Treatment with Ejiao successfully increased muscle mass, reduced oxidative stress, and improved overall locomotor activity. It achieved this by modulating the AKT/mTOR/Foxo3a and AMPK pathways.
Evidence Level: Preclinical (animal).
Important: All four studies above are preclinical — conducted in animals, insect models, or cultured cells. None currently constitutes direct evidence of a human treatment effect. They are cited here for mechanistic understanding, not as a basis for any specific human therapy or supplement claim.
10. Common Myths & Mistakes About Muscle Loss
Myth: "FoxO is always bad for muscle." Reality: FoxO is context-dependent. It drives destructive atrogene expression during illness and disuse, but the same FOXO activation is required for exercise to suppress DEAF1 and restore healthy mTORC1 signaling in aging muscle.
Myth: "More mTOR activity is always better for muscle." Reality: mTORC1 needs to be dynamically regulated. Chronic, unregulated overactivation — as seen in aged muscle with elevated DEAF1 — impairs autophagy and contributes to muscle senescence rather than growth.
Myth: "Maximizing autophagy through extended fasting is universally good for muscle." Reality: Muscle stem cell research shows both too little and too much autophagy (via DEAF1 dysregulation) impair muscle regeneration. Balance, not maximization, is the goal.
Myth: "Muscle loss during a hospital stay is just weakness from not moving — it'll come back on its own." Reality: Sepsis-driven muscle wasting involves active, coordinated molecular signaling (FoxO1/3a, NF-κB, suppressed mTOR) that actively degrades muscle tissue — it's a distinct biological process from simple disuse, and recovery often requires structured rehabilitation.
Myth: "A supplement that affects these pathways in a rat is proven to work in people." Reality: Preclinical signaling data (like the Ejiao study) is scientifically valuable and hypothesis-generating, but it is not equivalent to human clinical trial evidence. Treat such findings as promising leads, not proof.
11. Frequently Asked Questions
1. What causes muscle atrophy in sepsis? Sepsis-induced muscle atrophy is driven by a coordinated increase in FoxO1/3a and NF-κB signaling combined with suppressed mTOR activity, which together activate the ubiquitin-proteasome system, autophagy, and calpain-mediated protein breakdown in muscle tissue.
2. Can exercise really reverse muscle aging? Animal research published in PNAS in 2025 found that exercise suppresses a gene called DEAF1 through FOXO activation, which normalizes an overactive mTORC1 pathway and reduces markers of muscle aging in mice. Human trials of exercise's muscle benefits are extensive and well-established; this study adds mechanistic detail about why it works.
3. What is DEAF1 and why does it matter for muscle? DEAF1 is a FOXO-regulated transcription factor that controls both mTOR gene transcription and autophagy-related gene expression. When DEAF1 rises with age, it drives mTORC1 into a chronically overactive state and suppresses the autophagy needed to clear damaged muscle proteins.
4. Is mTOR good or bad for muscle? Both, depending on timing. Short-term mTORC1 activation after resistance exercise or protein intake supports muscle protein synthesis. Chronic, unregulated mTORC1 overactivation — as seen in aging muscle — impairs autophagy and contributes to muscle decline.
5. Does NF-κB only matter during infection? NF-κB is most strongly implicated in inflammation-driven muscle loss (sepsis, chronic inflammatory disease), but it also plays a role in disuse atrophy, where blocking NF-κB alongside FoxO activity has nearly eliminated fiber atrophy in animal disuse models.
6. What is autophagy and is more of it always better for muscle? Autophagy is the cell's process for clearing damaged proteins and organelles. Research on muscle stem cells shows both insufficient and excessive autophagy (via too little or too much DEAF1) impair muscle regeneration — the goal is balance, not maximization.
7. What is Ejiao, and does it actually help with sarcopenia? Ejiao is a traditional Chinese medicine preparation made from donkey-hide gelatin. In a rat model of sarcopenia, it increased muscle mass and reduced oxidative stress via modulation of AKT/mTOR/Foxo3a and AMPK signaling. This is preclinical animal evidence, not a confirmed human treatment.
8. How quickly can muscle be lost during critical illness? Muscle loss during sepsis and critical illness can begin within the first days of ICU admission and progress rapidly, which is why early mobilization and nutritional support are prioritized in modern critical care protocols.
9. Are there drugs available now that target FoxO, NF-κB, or mTOR for muscle wasting? Not as approved, muscle-wasting-specific therapies for humans as of this writing. Most of the pathway-targeting research described here — including the MuRF1 and DEAF1 findings — remains in the preclinical (animal/cell) stage. Current human-approved interventions for muscle wasting center on nutrition, physical therapy, and treating the underlying illness.
10. What's the single most evidence-backed way to prevent age-related muscle loss? Regular resistance training combined with adequate dietary protein remains the most robustly human-evidence-supported strategy, and the newest mechanistic research (the DEAF1 studies) helps explain the molecular "why" behind that long-standing recommendation.
11. Can diet alone reverse sarcopenia without exercise? Diet plays a meaningful supportive role — particularly adequate protein and possibly compounds affecting AMPK/FoxO3a signaling — but current evidence consistently shows resistance and aerobic exercise are the primary drivers of muscle preservation and regeneration in aging.
12. Should I take supplements that claim to target these pathways? Be cautious with any supplement marketed around "FoxO," "mTOR," or "autophagy" claims. Much of the underlying research is still preclinical. Discuss any supplement, including traditional remedies like Ejiao, with your physician before starting, especially if you have chronic illness or take other medications.
12. Conclusion & Action Steps
Muscle atrophy — whether from sepsis, aging, or inactivity — isn't a mystery anymore. It's the downstream result of a small, identifiable signaling network: FoxO1/3a and NF-κB driving breakdown, mTOR driving (or, when chronically dysregulated, undermining) growth, and autophagy clearing the cellular debris in between. The newest research adds real precision to this picture — from the FoxO-DEAF1-mTORC1 axis that explains why exercise reverses muscle aging, to the coordinated FoxO/NF-κB/mTOR signature behind sepsis-induced wasting.
Your action steps:
If you or a loved one is facing hospitalization or critical illness, ask the care team about early mobilization and adequate protein/calorie delivery from day one.
If you're over 40, start or maintain a resistance-training routine at least twice weekly — the single most evidence-backed lever you have.
Add regular aerobic activity; it appears to matter for muscle-gene regulation, not just cardiovascular health.
Be skeptical of any supplement claiming to "target autophagy" or "activate mTOR" without human clinical trial data behind it — ask your doctor first.
Revisit this article as new human trials emerge; preclinical signaling research like this often takes years to translate into approved therapies, but it reliably points toward where those therapies will eventually come from.
This article is for educational purposes and does not constitute medical advice. Always consult your physician or a qualified healthcare provider before starting a new exercise program, supplement, or making changes related to a diagnosed medical condition.
13. Sources & References
Fu, D., Zhou, M., Zhang, Y., Cheng, P., Shu, Y., Xiao, Q., & Zhang, M. (2026). Targeting FoxO1/3a, NF-κB, and mTOR signaling attenuates muscle atrophy in sepsis. Scientific Reports. https://doi.org/10.1038/s41598-026-52665-7
Choy, S.M., Goh, K.Y., Lee, W.X., Jiang, W., Gou, Q., Gopal Krishnan, P.D., Chee Ong, S., Chua, K., Harmston, N., & Tang, H.W. (2025). Exercise suppresses DEAF1 to normalize mTORC1 activity and reverse muscle aging. Proceedings of the National Academy of Sciences, 122(48), e2508893122. https://doi.org/10.1073/pnas.2508893122
Goh, K.Y., Lee, W.X., Choy, S.M., Priyadarshini, G.K., Chua, K., Tan, Q.H., Low, S.Y., Chin, H.S., Wong, C.S., Huang, S.Y., Fu, N.Y., Nishiyama, J., Harmston, N., & Tang, H.W. (2024). FOXO-regulated DEAF1 controls muscle regeneration through autophagy. Autophagy, 20(12), 2632–2654. https://doi.org/10.1080/15548627.2024.2374693
Zhang, H., Liu, S., Feng, Q., Liu, H., Wu, J., Duan, X., Li, Z., Zhang, Y., Zhou, X., Yv, M., Liu, C., Cheng, J., Du, G., & Zhao, L. (2025/2026). Ejiao alleviates sarcopenia by AKT/mTOR/Foxo3a and AMPK pathways in an aging rat model induced by D-Galactose combined with restricted movement. Journal of Ethnopharmacology, 356, 120819. https://doi.org/10.1016/j.jep.2025.120819
Duke-NUS Medical School. (2025, December). Why muscles weaken with age — and how exercise fights back. Duke University School of Medicine News.
Nakazawa, H., et al. Sepsis-associated skeletal muscle wasting is ameliorated by pharmacological inhibition of the STAT3 signaling pathway in mice. Scientific Reports (2026). https://doi.org/10.1038/s41598-026-35815-9
Reed, S.A., et al. Inhibition of IkB kinase alone or in combination with FOXO blockade eliminates disuse muscle fiber atrophy. Discussed in: Forkhead Box O Signaling Pathway in Skeletal Muscle Atrophy, American Journal of Pathology (2022). https://www.sciencedirect.com/science/article/pii/S0002944022002863
Bodine, S.C., & Baehr, L.M. Skeletal muscle atrophy and the E3 ubiquitin ligases MuRF1 and MAFbx/atrogin-1. American Journal of Physiology-Endocrinology and Metabolism.
Yang, Y., et al. Signaling Pathways That Control Muscle Mass. International Journal of Molecular Sciences, 21(13), 4759 (2020). https://www.mdpi.com/1422-0067/21/13/4759
Zeng, Z., Liang, J., Wu, L., Zhang, H., Lv, J., & Chen, N. Exercise-Induced Autophagy Suppresses Sarcopenia Through Akt/mTOR and Akt/FoxO3a Signal Pathways and AMPK-Mediated Mitochondrial Quality Control. Frontiers in Physiology (2020). https://doi.org/10.3389/fphys.2020.583478
Chen, R., Zheng, Y., Zhou, C., Dai, H., Wang, Y., Chu, Y., & Luo, J. N-Acetylcysteine Attenuates Sepsis-Induced Muscle Atrophy by Downregulating Endoplasmic Reticulum Stress. Biomedicines, 12(4), 902 (2024). https://doi.org/10.3390/biomedicines12040902
Sartori, R., Romanello, V., & Sandri, M. Mechanisms of muscle atrophy and hypertrophy: implications in health and disease. Nature Communications (2021).
Sandri, M. Protein breakdown in muscle wasting: role of autophagy-lysosome and ubiquitin-proteasome. International Journal of Biochemistry & Cell Biology (2013).
Bodine, S.C., et al. Akt/mTOR pathway is a crucial regulator of skeletal muscle hypertrophy and can prevent muscle atrophy in vivo. Nature Cell Biology (2001).
Sanchez, A.M., Candau, R.B., & Bernardi, H. FoxO transcription factors: their roles in the maintenance of skeletal muscle homeostasis. Cellular and Molecular Life Sciences, 71, 1657–1671 (2014).
Attaix, D., & Baracos, V.E. MAFbx/Atrogin-1 expression is a poor prognostic marker in cancer cachexia. Current Opinion in Supportive and Palliative Care (2010).
Puthucheary, Z.A., et al. Acute skeletal muscle wasting in critical illness. JAMA (2013).
Cruz-Jentoft, A.J., et al. Sarcopenia: revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31 (2019).
Han, X., Goh, K.Y., Lee, W.X., et al. Adult stem cells at work: regenerating skeletal muscle. Cellular and Molecular Life Sciences, 76(13), 2559–2570 (2019).
National Institute on Aging. Sarcopenia with Aging (patient/consumer information page).
World Health Organization. Sepsis fact sheet.
Schiaffino, S., Dyar, K.A., Ciciliot, S., Blaauw, B., & Sandri, M. Mechanisms regulating skeletal muscle growth and atrophy. FEBS Journal, 280(17), 4294–4314 (2013).